Working in partnership with people and communities is at the heart of our approach in South West London. By listening to local feedback and involving communities in the design of our work, we strengthen accountability and create meaningful opportunities for people to influence and improve the services they use.
Gaining insight into the needs of our diverse communities — particularly those experiencing health inequalities — alongside understanding people’s experiences of care, is vital to improving health services and supporting the prevention of illness.
In this section we describe:
- Our engagement strategy and legal duty
- The six different ways we engaged communities last year – with examples given across boroughs.
- The infrastructure that supports our engagement
- How we work with our local Healthwatch organisations and the voluntary, community and social enterprise (VCSE) sector
1. Our engagement strategy and legal duty
Our people and communities strategy supports us to ensure the voice of people and communities is central to all levels of our work – and that we have inclusive ways of reaching and listening to our diverse populations. Through our work we aim to:
- Reduce health inequalities by better understanding the needs and aspirations of our local people and communities and responding to them in how we plan and deliver services.
- Plan how local people and communities will be involved early – at the start of any work looking to change how services are delivered.
- Work with community leaders to strengthen our understanding of our communities and their experiences.
The NHS has a statutory duty to involve the public in decision-making, as set out in the Health and Care Act 2022. We are required to ensure that patients, carers and communities are involved in planning services, developing and considering proposals for service change, and in decisions that affect how services are delivered.
Building strong relationships with communities and engaging openly about proposed changes helps us meet these responsibilities. Listening to people’s experiences and perspectives is essential to designing services that respond to local needs. The scale and approach to engagement are proportionate to the significance and potential impact of each proposed change.
We work closely with Health Overview and Scrutiny Committees across our borough councils to plan and deliver engagement activity, helping to ensure that the views and priorities of local people remain central to decision-making.
1.1. Examples of key projects that influenced decisions/specifications
Engagement with people and communities informed a range of decisions and work across South West London this year. For example:
- Crisis cafe engagement – speaking with carers and service users to inform the development of our South West London-wide specification and involving people with lived experience in the procurement process.
- Engagement work in Sutton to better understand how behavioural needs develop in primary-aged children and how families with children with suspected or diagnosed neurodiversity can be supported earlier. Insights were used to refresh the Sutton Health and Care Plan and influenced the design of a public-facing neurodevelopment pathway and support map
- Outreach work in New Addington, Croydon, to understand more about local people’s experiences of health and care – which directly informed the development of the proposed Community Diagnostics Centre (CDC).
- Outreach work in Merton and Wandsworth, which helped us to understand the challenges people face when accessing dental services and maintaining dental hygiene. This fed into a targeted dental campaign and informed the planning of dental services across South West London.
- In Richmond, the insight gathered around alcohol consumption underlined the need for dedicated support for GP practices to provide early identification and brief interventions in primary care. It is informing the development of an alcohol locallycommissioned service for Richmond GP practices.
- The South West London anti-racism report contained key recommendations, co-designed with funded organisations, on how we develop an actively anti-racist health and care system across the six boroughs.
- Spring outreach work with communities experiencing health inequalities helped us understand people’s experiences of accessing health services. It led to targeted work to further understand how language barriers affect access to care with communities who have English as a second language
2. The six different ways we engaged communities last year in South West London and across our six boroughs
We use a range of complementary approaches to involve people and communities in shaping services. During 2025/26 these included six main methods:
2.1. Community-led approaches
Our community-led approach to engagement supports local people to shape conversations and influence priorities from the outset. Tailoring our approach to the needs of different communities helps build sustainable relationships between health, care and voluntary sector organisations, while supporting improvements in local health and wellbeing.
Across each borough, we have mapped the communities we need to reach to better understand those experiencing health inequalities, as well as the networks and communication channels that connect with them. These include local forums, community groups, social media and newsletters. We maintain regular engagement with community leaders throughout the year to understand what matters most to local people, share opportunities to get involved, and demonstrate how community insight has informed our work.
During the year, we worked in partnership with voluntary, community and social enterprise (VCSE) organisations to gather deeper insight and reach people whose voices are not always heard. This included a range of grant-funded initiatives aligned to the three shifts set out in the NHS 10-Year Plan, such as our Spring Healthy Communities Engagement Fund and Digital and Health Fund.
2.1.1. Understanding people’s experiences of accessing care through our Spring Grants work
Our healthy communities grants programme engaged 6,019 residents across South West London. Through this work, we gathered valuable insights into people’s experiences of accessing NHS services and maintaining healthy lifestyles.
With a particular focus on Core20 and other underserved communities, we explored the drivers of health inequalities, also putting a specific focus on understanding residents’ behaviours impacting health in each borough.
- In Croydon we focused on understanding residents’ access to NHS services, healthy lifestyle behaviours and views on mental wellbeing, a key priority in the Local Joint Health and Wellbeing Strategy.
- Kingston focused on hypertension which affects over 23,000 residents in the area.
- Groups in Merton focused on cardiovascular disease, one of the leading causes of preventable deaths leading to avoidable pressures and costs on the health and care system.
- Richmond’s focus was on behaviours around alcohol consumption with one in three adults in the borough drinking more than 14 units of alcohol per week, which is higher than both London and England averages.
- Cardiovascular disease was also a focus in Sutton where we funded 13 local organisations to deliver 28 activities, engaging with 25 different ethnic groups across the borough’s four integrated neighbourhood teams.
- Wandsworth’s groups had in-depth conversations to understand respiratory health, which is a significant concern due to high emergency admissions for chronic obstructive pulmonary disease (COPD) and lower respiratory tract infections in children. Smoking is a leading cause of death in Wandsworth, with young people more than twice as likely to smoke at age 15 than their peers across London.
In total, we awarded grants to 87 local VCSE organisations to facilitate conversations at trusted community settings and events. By working with established local partners, we were able to reach individuals who may not typically participate in NHS engagement activities, including residents whose first language is not English.
While these grants were running, the national NHS 10-Year plan was published. To support the development of neighbourhood working, we firstly analysed our data across the boroughs. We then provided a further breakdown of our analysis of insights by neighbourhood to allow teams find out what is important about health care provision in their specific localities.
This work resulted in a vast collection of insight from participants from diverse ethnic, socio-economic and health backgrounds across South West London. Our findings have been shared at neighbourhood-level, helping to guide local interventions to improve prevention, access and equity in health services. Insights are also being used by integrated neighbourhood teams and long-term conditions steering groups to guide person-centred service design and address health inequalities.
“Everything needs to be culturally sensitive, if I can’t see the food that I eat in the guidance, then it’s not for me.” – Wandsworth
“There’s a fear of being over-medicalised, like they’re quick to give us pills rather than understand what’s going on.” – Merton
“Those with mental health problems do not often go to the GP as they fear being judged, of stigma and feel too proud to go to see someone” – Sutton
“There doesn’t seem to be enough connection between the surgeries and the hospitals in Richmond.” – Richmond
“My impression is that NHS is often too slow and time-consuming. I only wait until there is a major/serious health issue.” – Kingston
”It would be useful to have an awareness campaign so that people know where they can go to see what services are available.” – Croydon

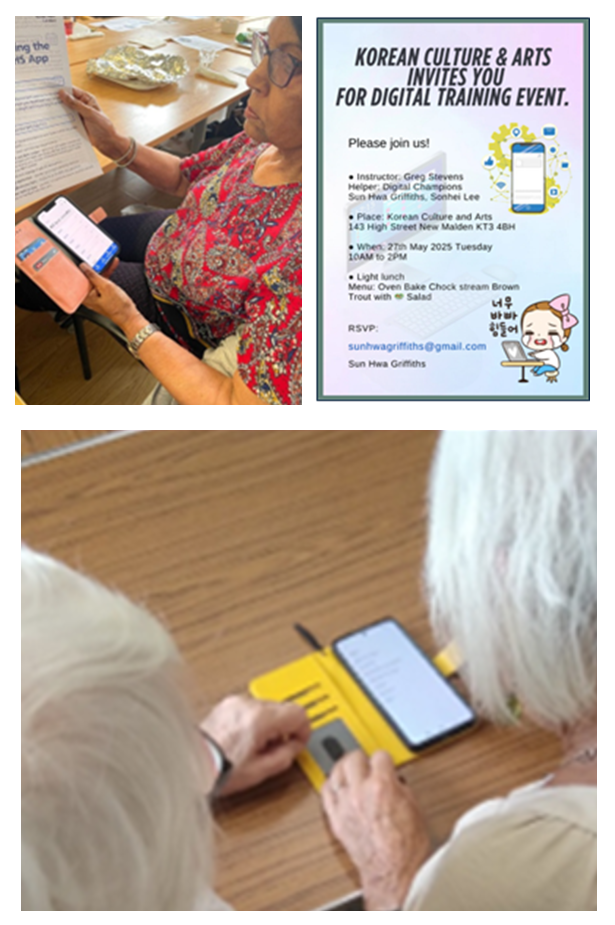
2.1.2. Understanding how technology can improve access to care through our Digital and Health Fund
The Digital and Health Fund focused on understanding how technology can improve access to care. It aimed to find out about potential digital barriers that people living in South West London might face so that we could enable people to be ready for digital change. This included increasing digital uptake and use of the NHS App and finding out how people felt about technologies and ambient artificial intelligence.
Working with our CVS umbrella organisations in each borough, we funded 26 local voluntary, community and social enterprise (VCSE) organisations, which support our Core20 populations, to deliver a total of 82 activities. These included in-depth conversations with 983 people from a range of ethnicities, socio-economic and health backgrounds. The insight gathered will help to shape our providers’ digital strategies, transformation programmes and investments including a business case for ambient voice technology in our four acute hospitals.
“If these apps help us take care of ourselves, why aren’t we being shown how to use them?”
“I am against artificial intelligence because it is not a living being – it cannot understand emotions or accents.”
“Better research for the NHS, like symptoms you have.”
“More information online rather than waiting”
“Less paper-based because all information is at your finger-tips.”
2.1.3. Women’s health education grants
Kington and Richmond NHS Foundation Trust colleagues from women’s health, physiotherapy, genitourinary medicine and the trust’s patient experience and involvement team attended seven women’s health events. These included groups for Tamil women, migrants and young people, and were hosted by community organisations – Malarum Ithayangal (Tamil group), Voices of Hope, Migrant Advocacy Service, Ukrainian Social Club and Places Leisure (girls 9 to 15). The events were supported by NHS South West London ICB’s Women’s Health Education grants.
These sessions highlighted significant gaps in access to basic women’s health information, including the absence of words for some body parts in certain languages and difficulty finding menopause information and support. Insights from this work will help shape the design of women’s health services across Kingston and Richmond.
2.2. Listening events
We want to have a continuous conversation with local people about what matters to them.
2.2.1. Community leaders’ event
We ran an event on the 18 March 2026 with our community leaders. It brought together over 80 community and voluntary sector organisations from across our six boroughs for a listening event focused on community insight and neighbourhood working.
Led by Dr Anne Rainsbury and Dr Andrew Murray, the session built on January 2025 engagement linked to the 10 Year Health Plan and included examples from Kingston and Croydon to show how services are starting to work differently at neighbourhood level.
Most of the session was spent in table discussions, where place leads supported conversations on what people are seeing and hearing in their communities and how we can strengthen neighbourhood teams, build more partnerships with VCSE organisations, and work better together to deliver joined-up care.
Across the discussions, there was a clear call for more equal partnership with VCSE organisations, better visibility of services, and a focus on turning insight into action.
As well as giving us insight in how we work well with the sector, and where improvements could be made, this will help shape our work as we develop our clinically-led strategic plan (CLSP).

2.2.2. Anti-racism conference
More than 60 people attended the South West London anti-racist approach conference on Wednesday 28 May 2025, hosted by Croydon Vision. The conference provided the opportunity for the funded organisations to come together to share insight gathered through their engagement and help shape recommendations. The insight from this conference has been included in the main findings section of this report. This work empowered grassroots and voluntary organisations to lead local engagement work and co-design actionable recommendations with global majority communities most impacted by health inequalities. Key recommendations, co-designed with communities, will support the development of an anti-racist framework for all health and care systems within South West London.

“The recommendations from the report of this research intends to be hard-hitting and far reaching and to be used by health providers across the health and care sector to deliver equity to communities they serve.” John Azah OBE Chief Executive, Kingston Race and Equalities Council (KREC)
2.3. Partnership working with partners, VCSE organisations and Healthwatch
The Integrated Care System brings health and care organisations closer together than ever before – so collective resources can be used to meet people’s needs most effectively. There is a greater focus on working with voluntary and community organisations and our six Healthwatch organisations across South West London. We have a united ambition to foster our existing relationships with local people and work with our diverse people and communities across our six boroughs, so we can make a bigger collective impact by collaborating on programmes of work.
2.3.1. Outreach in New Addington to inform the development of a community diagnostic centre
We undertook a programme of outreach in New Addington, Croydon, to understand more about local people’s experiences of health and care. The engagement also had the aim of informing the development of the proposed community diagnostics centre (CDC) in the area. New Addington is one of Croydon’s Core20 areas where reducing health inequalities is a priority.
To complement the outreach in New Addington, we commissioned Healthwatch Croydon to engage local people to better understand their experiences and the potential needs of the area. As well surveying 50 residents of New Addington, Healthwatch Croydon engaged 120 people who had used the Purley CDC to find out about their understanding of CDCs and their experiences of using the service.
We engaged with local residents, community leaders, organisations and volunteers at New Addington community locations to capture a range of insights. the New Addington Community Facilitator for Croydon Voluntary Action helped us identify opportunities to engage with residents. Two organisations– New Addington Pathfinders and The Family Centre ran focus groups and one to one conversations to understand people’s experiences.
Both NHS South West London and Healthwatch Croydon produced insight reports highlighting the key themes and recommendations to inform the development of the CDC. Working in partnership using a variety of engagement techniques painted a well-rounded picture of the experiences of New Addington residents and their needs.
“There are 22,000 people living in New Addington and we are 8.5 miles from the nearest hospital – we need these services.”
2.3.2. Engaging with carers to inform Richmond Carers charter
Over the last year, we worked collaboratively with local health and care partners including Healthwatch Richmond, Richmond Carers Centre, Richmond Council and Richmond CVS to co-produce a new Adult and Young Carers’ Charter, a shared boroughwide commitment to recognising unpaid carers across Richmond.
The charter is informed by engagement where more than 250 adult and young carers shared their experiences. Carers described feeling invisible, facing financial strain, and struggling to access timely local support.
Their feedback directly shaped the charter’s four priorities: improving recognition and understanding of carers’ expertise and responsibilities; reducing financial, employment and educational challenges; creating carerfriendly services and communities; and improving health and wellbeing through better access to breaks, social connection and flexible appointments. These shared priorities provide a clear framework for local statutory and voluntary organisations to work together to ease the pressures carers face and ensure they are valued, heard and supported.
Building on the themes captured in the carers charter engagement, we carried out one-to-one interviews to gather further insight into the pressures carers face and the improvements they would like from local health services.
Carers spoke about the impact of long waits, difficulties accessing specialist mental health support, the emotional and financial strain of caring, and the frustration caused by poor coordination between services. Many also highlighted how hard it is to find clear information or receive proactive signposting, even though they valued support from local organisations once they discovered it. These insights will help ensure carers’ voices can shape local health and care plans and future neighbourhood programmes.
2.3.3. Healthy teeth and smiles – understanding people’s day-to-day oral health habit in Merton and Wandsworth
Poor oral health remains a significant challenge in South West London. It is closely linked to wider health inequalities, poverty, disability and ethnicity. Oral disease has an impact on eating, speaking, sleeping and school readiness in children and health conditions later in life. Locally, organisations have raised significant and growing concerns about rising problems with oral health, particularly among those on low incomes.
We worked closely with Merton Connected and Wandsworth Care Alliance, the umbrella organisations of the VCSE groups in Merton and Wandsworth, to help us understand people’s day-to-day oral health habits, barriers to maintaining good oral health and the cultural, emotional and financial factors shaping their behaviours. This work prioritised our Core20 and underserved communities, where people often face the greatest inequalities and poorest outcomes.
We funded 15 voluntary and community sector organisations with grants of up to £2,000 to run focus groups and community research across the two boroughs. Over 970 people took part across 89 activities, including children and young people, older people receiving care at home, disabled and neurodivergent people, refugees, people experiencing homelessness and those living in temporary accommodation.
This insight has helped us understand the role of prevention and where support should be targeted. We worked with the South West and South East London dentistry leads to inform the programme development. Throughout the process we also worked to raise awareness of the school teeth brushing programme which operates in nursery and primary schools across South West London. NHS England has also reviewed the NHS Choices website to improve visibility of practices accepting? new patients. The insight directly influenced our South West London urgent dental care campaign – see below for more details.
“We can’t afford electric toothbrushes for the whole family.”
“The nearest dentist to our building was closed last year… now it’s in Morden – too far with my walking stick”
“Flossing or brushing makes me gag. They don’t understand – they think I’m gross.”
“I wasn’t sure if I would be eligible to use 111 because of my immigration status.”
“If you had a tooth care package like you do with glasses and opticians – that would help a lot.”

2.4. Focus Groups, interviews and community events
We often bring together small groups of people to hear about particular health topics or to hear from specific communities to inform our work and help shape local health and care services. Sometimes it will be more effective to talk to people on a one-to-one basis and this is often used to complement insight gathered from a focus group or survey. We aim to speak to specific communities based on what our local data and insight tells us about who is or isn’t accessing services, people who have poorer experiences of services and those with poorer health and wellbeing outcomes – aiming to make sure we hear from people that are representative of the population in South West London.
2.4.1. Understanding how language barriers affect access to care in South West London
In autumn 2025, we worked with local community organisations to better understand how language barriers affect access to primary care across South West London. This work built on insights from our spring 2025 engagement programme, where language barriers were raised as an issue for many in our Core20 and underserved communities. To explore these issues in greater depth, we worked with community organisations, funded through the Spring Engagement Fund, that had identified language as a key issue, to deliver small group discussions and one-to-one conversations.
We engaged with communities across the six boroughs whose primary languages included Urdu, Somali, Spanish, Punjabi, Cantonese, Mandarin, Hindi, Korean, and Portuguese. Language barriers were an issue throughout the patient journey, including difficulty booking appointments and understanding clinicians during consultations. Participants said these barriers contributed to delayed access to care and increased reliance on family members or friends to interpret, which in some cases resulted in inaccurate or incomplete information and difficulties discussing personal or sensitive health issues. The insights gathered through this engagement will help to inform future work to improve access for people who don’t speak English as their first language and will be shared with the communities involved.
2.4.2. Improving emotional wellbeing for children and young people in Sutton
We carried out engagement to understand how behavioural needs develop in primary-aged children and how families with children with suspected or diagnosed neurodiversity can be supported earlier. The report can be found here.
To reach as many families as possible, we used a layered engagement approach, working with schools, partners and families to shape our approach. This included a school coffee morning, one-to-one interviews and a survey of parents. Parents described difficulties navigating the system, particularly understanding what support is available without a diagnosis due to system delays, and highlighted how masking behaviours can create barriers to getting a diagnosis. These insights are being used to refresh the Sutton Health and Care Plan and to shape ongoing work on SEND and CAMHS services, This work included supporting South West London and St George’s Mental Health NHS Trust to design a pathway map, which takes parents and carers through the support vailable to them and the process for getting an assessment and diagnosis.
2.4.3. Understanding the barriers faced by people experiencing homelessness and how services may better meet their needs in Merton
In Merton, 3,398 people have applied for support with housing and homelessness since 2018. There is a significant divide between east and west Merton. Some 73% of applicants coming from East Merton, reflecting wider inequalities including poor housing conditions, higher deprivation and poorer health outcomes. Housing insecurity is closely linked to increased risks of physical and mental health problems, making timely access to healthcare vital, yet challenging for many people.
We wanted to understand the barriers faced by people experiencing homelessness and how services may better meet their needs, linked to the Mayor of London’s plan to end rough sleeping.
In August 2025, we worked with a local partner and night shelter, interpretation services and the Merton Connected Social Prescribing team to make the most of the opportunity to share learning and strengthen connections.
Through our focus group with 10 residents we found that people were unsure how to register with a GP, that a lack of translated information made it hard to communicate needs and navigate the system. Digital exclusion and confusion over entitlements and charges for NHS services also played a part in the poor health outcomes for residents. We heard that many avoided health services altogether other than A&E which often felt like the only option, especially for work related injuries.
We have shared the insights we gathered with Merton’s health and care providers to help them plan ways to improve services for this vulnerable population – and reported our findings to the Merton Health and Care Place Committee.
We also arranged for an NHS 111 outreach team to attend night shelters to inform residents of the service to help them get the right help at the right time.
Specific findings about access to dental care have been included in an overarching Merton and Wandsworth Oral Health report which has been shared with the South West London Local Dental Committee, Merton and Wandsworth Primary Care and Community Care team, NHS England Public Health colleagues and with our partners at King’s College Community Special Care Dentistry team to inform future service planning and support.
You can read more about our findings and the impact of this insight here.
“I don’t always look at my phone and I might be in good health one day and the next day I’m not – what do I do then if the GP won’t ring me back?”
“It took me 25 minutes to walk from the bus stop to the dermatology ward for my appointment, but I’m too embarrassed to ask to use a wheelchair”.
“[If I had toothache] I would just go to the pub, it worked when I had the flu”.
2.5. Digital and online engagement
2.5.1. Engaging with people with lived experience to inform the development of a SWL specification for crisis cafes
To help inform the development of a new specification for crisis cafes across South West London, we undertook a programme of engagement during August and September 2025. This piece of work sought to ensure that local people can expect the same high quality of care no matter where they live. We wanted to ensure that the service specification was informed by service users, potential service users and carers. We started by conducting a desk top review of existing insight – it highlighted the need for more information about: location of cafes; opening times; awareness of the service; activity preference and accessibility needs.
To meet this gap in insight and to enable people to take part in multiple ways, we shaped the specification using a mixed methodology that supported insight from service users, those who don’t access the service and those who experience poorer health outcomes.
We developed an online survey, open to all, to enable a higher volume of people to share their feedback. This was promoted by partners, providers, VCSE contacts and via social media. In recognition that surveys have limitations in who they reach, this was complemented by a more targeted approach through semi-structured interviews, promoted via VCSE networks and through the survey.
We prioritised speaking to a sample of people who are underrepresented in prevention services, such as people who have English as a second language, those from global majority backgrounds, and carers.
We also conducted one-to-one interviews with service users and carers. These were led by mental health commissioners, who attended crisis cafés to speak to service users or interviewed them by phone, where requested. We heard from over 270 people and their feedback directly informed the service specification – and continues to influence our transformation work for people in mental health crisis.
We also involved people with lived experience on the evaluation panel to assess the bids. To enable independent and impartial support, our South West London Healthwatch executive officer supported two people (who were paid for their time) through the training, evaluation and moderation process.
2.5.2. Engagement to inform the development of our adult ADHD pathway
As part of a review into how ADHD services are delivered for adults – we have been supporting the team to provide clear information and have planned engagement work to further understand people’s experiences.
We began by conducting an initial literature review into existing feedback about ADHD diagnosis and services. It showed that while there is rich insight about children’s services, there was less about adults. We are working with the team to develop an engagement approach to fill this gap in knowledge through an online survey and offer of telephone support. The survey launched ch 2026 and asked about people’s experiences of considering an ADHD assessment, accessing information and support, waiting for services, and receiving treatment. It also asks for views on how ADHD services could be organised and improved in future.
For adults, there is a lot of unofficial advice available on social media – particularly around Right to Choose assessments. However, there is little insight about people’s experiences while they wait for an assessment. To help provide clear and consistent information for patients and healthcare professionals, we have supported the team to develop a webpage on Right to Choose.
2.5.3. Supporting winter pressures through WhatsApp networks
In previous years we have heard from our community groups that WhatsApp groups are very widely used in our boroughs. Indeed, we have heard through our insight that many people use WhatsApp groups as their main source of information.
We are also aware that some of our residents are unable to read in their home language so we have worked with communities to design a way of ensuring that our messages are shared with people for whom this is a barrier to information.
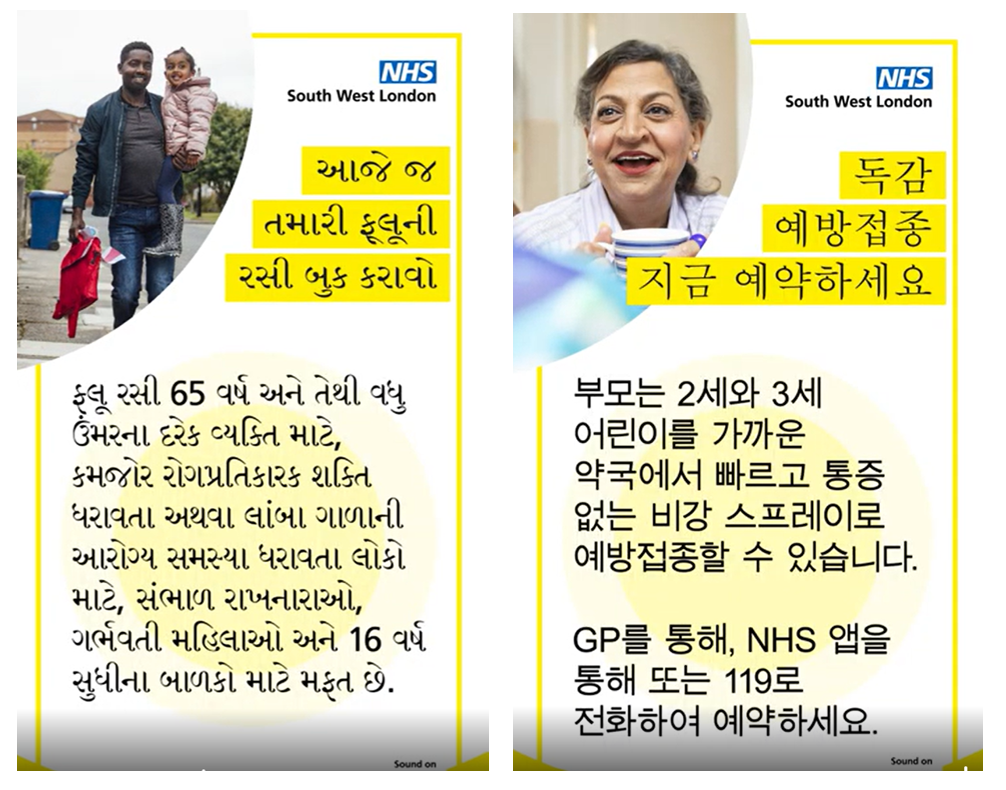
To support winter messaging this year, we shared translated voicenotes from local clinicians and community leaders encouraging people to take up the offer of vaccines; informing them of pharmacy services and telling them where to go for help when our services were very busy.
Community groups shared these messages through their own networks and encouraged forward sharing. This improved more equity in how people accessed information across South West London with no one left behind.
2.6. Communications and engagement campaigns
We use a community engagement-centered approach to sharing information and raising awareness of services, working through the wide-reaching networks built by our borough engagement leads and their strong relationships with community leaders and voluntary sector organisations.
We work with groups and individuals to share the information which is most relevant, or of most interest .Feedback from local people helps develop our messaging.
Building on our community engagement, we also share information through many public facing channels and ask our trusted partners to share materials on our behalf – for example, through websites, social media channels, staff communications networks and community and stakeholder newsletters. We also use paid marketing – such as radio adverts, outdoor advertising and digital advertising. This is how we ensure information is reaching individuals through lots of different routes.
Our approach to communications and engagement campaigns is based on this ‘integrated approach’ where we adapt our consistent messages and materials to suit each targeted audience. This means bespoke communications for our diverse communities, around geographies, age, ethnicity, but also for staff and for different digital platforms.
We use a behavioural science approach so we can truly understand our audience and engage with them in the right way. Our aim being to help people make good choices with accurate information.
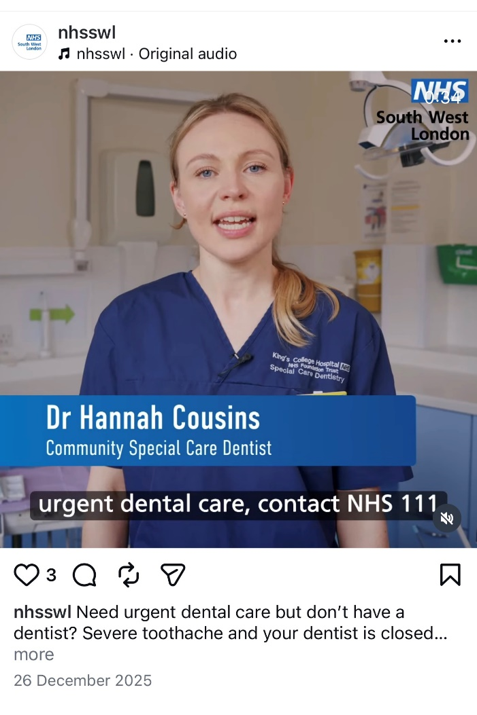
This year, we have run a range of priority campaigns – promoting dentistry, Pharmacy First and vaccines and immunisations. Here is a summary
Dentistry – The campaign was seen online 4,097,443 times in a six-week period, with an engagement rate of 6.7% (five times our average engagement rate for similar campaigns). Most importantly, we saw an increase in the number of urgent appointments booked, by up to 37%. particularly in the areas of greatest deprivation where our targeting was concentrated.
Pharmacy First – paid online advertising promoting pharmacy services and the support they offer. People are up to four times more likely to visit a pharmacy once they’ve seen one of the borough-specific adverts. Last year, referrals to the Pharmacy First scheme increased by 41% during our campaign. This campaign was viewed over 500,000 times in the first month.
Vaccinations and Immunisations – our flu campaign was seen 12.4 million times on and offline, targeting areas of low uptake – this means it was seen 47% more times than last year. It generated over 76,000 clicks to book. We developed new materials in partnership with GESH featuring ITU consultants talking about rising flu rates. Materials in different languages reached new audiences with Urdu, Spanish and Polish being the most engaged with.
Our grant programmes underpin our campaigns and provide outreach and engagement in local communities, for further information see our Spring Grants Fund in the ‘community-led approaches’ section.
3. The infrastructure that supports our engagement
A key element of putting engagement at the heart of decision making is ensuring the voice of people and communities has an impact on strategic forums. Our decision-making framework is described as our governance, and we use a range of ways to ensure there is a strong presence for people and communities and their views.
3.1. Governance and leadership
Our Executive Director of Stakeholder and Partnership Engagement and Communications and Deputy Director of Communications and Engagement have responsibility for coordinating our engagement activity to maximise its impact as a key system priority and ensure that our work influences priorities and decision-making. For the majority of last year, we also funded two strategic posts, a South West London VCSE director (funding ended in October 2025) who supported collaborative working across six boroughs and an executive officer post for South West London Healthwatch which supports our six local Healthwatch organisations with partnership working.
We also have a South West London People and Communities Engagement Group which works collaboratively across the partnership to review engagement plans and activities, with membership from including medical directors and programme directors from our provider organisations.
For example, the group met in April to hear about our grant engagement programme and insight work at place. The group discussed how these reports will have an impact on the running, planning and design of services going forward. After each meeting, we report to the Integrated Care Board through our Chief Executive’s update and reports are published on our website.
We also attend the Patient Experience and Engagement Group, which comprises colleagues from quality and patient experience teams within trusts, to enable us to triangulate patient experience and engagement data. This gives us a more robust baseline to understand how to improve outcomes for patients. We also attend quality meetings at place to share insight work and feed in at a local level.
3.2. Representation at decision making forums
In all the key meetings where decisions are made, members are required to consider patient and public engagement and communications activity. This includes our Integrated Care Board and Integrated Care Partnership, which meet in public. Active consideration of the voice of our people and communities is a requirement of our constitution and implemented by our submission templates for papers. Our Integrated Care Board constitution states: “The Board will receive reports which provide an overview of the engagement activities across the Integrated Care Board – noting the communities it has reached, impact that it has made, decisions it has influenced and any lessons learned”.
People and communities are also central at our borough Place Committees, championed by all partners sitting round the table – including Healthwatch, VCSE representatives and Health and Wellbeing Board Chairs. When considering priorities and service transformation plans, lived experience and insights from the community focus discussions and are key to agreeing the way forward.
We work with a number of patient or public partner champions who are involved in our local decision making on our committees and meetings either at the borough or South West London level. A patient or public champion is often someone with lived experience who gets involved to represent their own views or works with local networks, our Maternity Voices Partnerships, for example, to advocate and make sure their voices are heard.
3.2.1. Network of communication and engagement professionals
We have professional communities in each of our six boroughs that bring together local authorities, NHS trusts, our borough engagement leads, the voluntary sector and Healthwatch. Through these networks we bring together insights and coordinate engagement activity at Place level so we can gain a more comprehensive picture of the views and experiences of local people and communities.
3.2.2. The South West London Bank of Engagement Insight
The South West London Insight Bank is a system-wide online approach to capturing, storing and reusing engagement insight to inform commissioning and service design. It brings together insight from across multiple agencies and engagement activities to reduce duplication, widen inclusion of under-represented communities, identify gaps in knowledge and reach, and ensure that patient and public views are consistently reflected in decision-making. It enables our programmes of work to understand what matters most to local people. The insight bank strengthens the link between engagement and commissioning decisions and improves transparency about how feedback is used. To date there are over 300 reports collated in the bank – providing colleagues with a rich baseline of data to inform their work. Visit the Bank of Engagement Insights
3.2.3. Toolkits and support
Our engagement toolkit supports colleagues to listen, build trust and embed involving local people and communities in their work. It includes ‘how to’ guides on: running a survey; focus groups; funding trusted local VCSE organisations; recruiting people with lived experience; evaluating research; mapping stakeholders and running an online event. It also offers ‘top tips’ for working with specific communities – which were codesigned with that population.
3.2.4. How people can get involved and how we share updates
Since April 2025 we have published 17 South West London reports on our insight bank. This demonstrates that our work is transparent and accountable to the public, but it also enables other organisations to access tour reports to inform their work.
For all our engagement activities we promote opportunities to relevant VCSE organisation, through our networks and contacts and via our Healthwatch organisations. We use organic and paid for advertising and promotion to support us to reach relevant groups of people. Opportunities are also published on the ‘get involved’ section of our website.
4. Working with our six Healthwatch organisations and the voluntary, community and social enterprise (VCSE) sector
4.1. Healthwatch
We have always worked closely with our six Healthwatches. As independent statutory bodies, they help us hear people’s feedback and improve standards of care. Their insight from people and communities has influenced what we do and how we run NHS services.
We have continued to fund an executive post – to support collaborative work and provide senior representation on key committees.
This year, Healthwatch colleagues carried out engagement to understand whether the move to a new commissioned BSL interpretation provider (DAL, introduced across GP practices from October 2024) had improved access for d/Deaf and deafblind people. The work built on earlier Accessible Information Standard (AIS) engagement and explored whether the service change addressed previously reported barriers across the patient journey.
Between April and June 2025, Healthwatch used a mixed-methods approach, including two focus groups, a patient interview, and engagement with GP practice staff via a short survey and feedback gathered through practice manager forums and a GP update event. In total, Healthwatch heard from a total of 38 people with relevant experience: 21 patients and carers and 17 GP practice staff.
Feedback highlighted that improving accessibility requires reliable, high-quality communication support throughout the pathway—booking, consultation, referrals and follow-up—in line with the AIS. Ongoing issues included interpreter reliability and late cancellations, communication needs not being carried into referrals, and patients having to repeatedly restate their needs. We are working with Healthwatch to review their recommendations and to see how it can inform the delivery and commissioning of this service.
4.2. Voluntary, community and social enterprise (VCSE) sector
Our voluntary and community partners play a vital role in helping us deliver our community-led approaches, broaden the diversity of participation, and build trust through ongoing dialogue.
For example, CVS groups across our six boroughs have partnered with the South West London Gynaecology Clinical Network to distribute £187,000 to grassroots organisations for the development of women’s health hubs. This is part of a national initiative to enhance women’s health services across the UK by supporting culturally appropriate and tailored education and self-management. It allowed local organisations to work with the most marginalised women in safe and familiar community settings through group sessions and training of community champions to empower local advocates of women’s health.
Our voluntary and community partners play a vital role in helping us deliver our community-led approaches, broaden the diversity of participation, and build trust through ongoing dialogue.
For the first part of 2025/6, the South West London VCSE Alliance worked together to nominate 12 VCSE representatives, each an expert in their field, to sit on strategic ICB partnership boards and working groups.
Their role is to contribute specialist insight to ensure that the VCSE perspective is embedded in our system discussions and help elevate key issues affecting the VCSE sector. These included the Integrated Care Board, Health Equity Partnership Group, SWL Mental Health Partnership Delivery Group, Children and Young and Young People and Maternity Partnership Group, Older People’s Delivery Oversight Group and the Integrated Care Partnership Workforce.
The contract for the South West London VCSE Alliance ended on the 30 September 2025 and due to the Management Cost Savings programme, we were unable to renew the contract immediately. However the CVS infrastructure groups decided to continue to meet monthly for the rest of the financial year. We have continued to update them on changes to the ICB and to work closely with them as strategic partners in health and care.
For example, a round table discussion in February was attended by over 40 representatives from the sector to look at ways we can work together to make sure mental health has parity with physical health as we implement the delivery of the NHS 10-Year Plan.
The work of local Healthwatches and voluntary and community sector partners has been essential this year. Without their contributions, our reach would have been more limited and the insights we gathered less comprehensive. Recognising the value of their roles, we continue to invest in partnerships and collaborative working across our six boroughs.