1. Performance report
1.1. Welcome and overview from Joint Chair and Chief Executive Officer
Welcome to the annual report for NHS South West London Integrated Care Board. This report is a record of our operation from 1 April 2025 until 31 March 2026.
This year has brought significant national change for Integrated Care Boards. The publication of the Model ICB Blueprint and the NHS 10-Year Health Plan set out how ICBs will work differently in future, with greater emphasis on neighbourhood services, prevention and long-term sustainability. At the same time, ICBs have been required to reduce running costs.
For South West London, these changes have taken place against the backdrop of continued pressure on services and growing demand for care. Throughout the year, our focus has remained on improving health and care for the 1.5 million people who live in Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth.
Our achievements
At the start of the year, the Board agreed three corporate objectives for 2025/26. These were to redesign the ICB in line with national requirements, to review and update our plans for the years ahead, and to focus our resources on the areas that will make the greatest difference to local people.
Neighbourhood health has remained central to this work. Across our six boroughs, integrated neighbourhood teams are bringing together general practice, community services, mental health services, hospitals, councils and voluntary organisations to provide more joined-up care, particularly for people who are frail or living with long-term conditions. This approach supports earlier intervention, better coordination and care closer to home.
This work has received national recognition. Croydon was selected as one of the first areas in England to take part in the national neighbourhood health roll-out, reflecting the strength of local partnerships and the progress already made in shifting care into the community. South West London was also chosen as one of seven systems nationally to take part in NHS England’s Frailty Discovery Collaborative. This programme focuses on improving care for older people, helping them remain independent for longer and reducing avoidable hospital admissions. The learning from this work will inform practice across all our boroughs.
During the winter period, we introduced an Integrated Care Co-ordination Hub across South West London. The hub connects ambulance crews directly with senior clinicians, helping identify patients who can be safely supported at home or through community services rather than attending emergency departments. This has helped manage winter pressures while ensuring people receive care in the most appropriate setting.
During the year, responsibility for a number of specialised services transferred from NHS England to ICBs. This includes services such as cancer care, specialist mental health and renal services. Taking on this responsibility allows us to plan care more coherently across whole pathways and strengthen oversight of quality and outcomes.
Through the Medium-Term Planning Framework, we have ensured that our plans are realistic and affordable. This careful approach to financial management is essential to protecting frontline services and maintaining safe, high-quality care.
Clinical leadership has remained central throughout. Clinicians across primary, community and hospital services have played a leading role in shaping neighbourhood development, service planning and our response to national reform. We have also strengthened our governance and leadership arrangements to support this next phase of change.
Challenges
National reform has reshaped the role of Integrated Care Boards and required reductions in running costs. In South West London, this has meant reviewing how we are organised and beginning a process of redesign. We recognise the uncertainty this has created and remain grateful to colleagues for their professionalism and commitment throughout this period.
The introduction of the national Medium-Term Planning Framework has provided greater clarity about how systems plan over more than a single financial year. This has supported a more consistent approach to prioritising resources and ensuring services remain affordable while maintaining quality and safety. We continue to face challenges with our estate. Some buildings are not suited to modern healthcare and require investment to support safe and effective care. Delays to major capital schemes mean that careful management and phased improvement are necessary to maintain standards.
The way we work
Strong partnerships remain central to how we deliver for local people.
We continue to work closely with our six local authorities, NHS trusts, primary care providers, Healthwatch and voluntary sector organisations to plan services around the needs of our communities. Clinical leadership and neighbourhood partnership working are key to this approach.
During the year, there were changes in Board leadership. Dr Anne Rainsberry served as Acting Chair from September 2025 to early February 2026, following the departure of former Chair Mike Bell, and continues as Deputy Chair for South West London. It was also announced in January that Katie Fisher was leaving her role as Chief Executive to take up a new interim position at NHS North Central and North West London ICBs.
In December 2025 the Board agreed to collaborate more closely with NHS South East London through a formal clustering arrangement. In February, Sir Richard Douglas was appointed as Joint Chair of both organisations, and Andrew Bland was appointed as the shared Chief Executive.
Both ICBs remain separate statutory bodies, with their own Boards and legal responsibilities. The new arrangements enable us to share leadership capacity, reduce duplication and strengthen strategic commissioning across south London, while maintaining local accountability within each area.
Looking ahead
As we move into 2026/27, our focus remains on delivering the ambitions set out in the NHS 10-Year Health Plan and embedding the role of the ICB as a strategic commissioner.
Neighbourhood health will continue to develop across all six boroughs, supporting more coordinated care closer to home and improving outcomes for people with long-term conditions and complex needs.
We will continue to ensure that services are financially sustainable and that public money is used responsibly. Through strong local partnerships and closer collaboration across South East and South West London, we remain committed to improving health and care for everyone who lives and works in South West London. As Joint Chair and Chief Executive, we are confident that closer collaboration across south London will strengthen our ability to plan and commission services that meet the needs of local people. While each ICB remains accountable to its own communities, working together allows us to share expertise and leadership in a way that benefits residents across both areas.
Richard Douglas, Chair

Andrew Bland, Chief Executive Officer
1.2. About us
Welcome to the annual report for NHS South West London Integrated Care Board. This report is a record of our operation from 1 April 2025 until 31 March 2026.
NHS South West London Integrated Care Board (ICB) is committed to the four core purposes of Integrated Care Systems:
- Improving outcomes in population health and healthcare
- Tackling inequalities in outcomes, experience and access
- Enhancing productivity and value for money
- Helping the NHS to support broader social and economic development
NHS South West London is dedicated to our role to lead and support our system and partners in the delivery of these four core purposes.
Our goal over the next five years is to enable South West Londoners to Start Well, Live Well and Age Well. Our ambition is to make real and tangible improvements in health and care for local people.
The ICB is a statutory organisation bringing together the NHS to improve population health and establish shared priorities for local people, as well as being responsible for deciding how the NHS budget for South West London is spent.
This annual report covers from 1 April 2025 to 31 March 2026.
NHS South West London serves over 1.5 million people across our six diverse boroughs:
- Croydon
- Kingston
- Merton
- Richmond
- Sutton
- Wandsworth
We are responsible for overseeing the annual South West London NHS System budget of £4,461 billion, which covers the costs of running the organisation as well as the NHS services commissioned for the local population. The majority of these NHS services are delivered in our six places, but some services will be commissioned from NHS organisations outside the South West London patch. These NHS services include hospital services, community services, mental health, learning disability services, continuing healthcare, local primary care services and prescribing.
The total South West London ICB budget covers expenditure with:
- South West London NHS providers (acute, community and mental health)
- Providers from outside of South West London
- Primary medical care (GP) services
- GP prescribing and other local primary care services including local incentive schemes
- All age continuing healthcare
- Dental, ophthalmic and pharmacy services
The South West London system is allocated an NHS capital budget which can only be used by NHS organisations. In 2025/26 this was £166 million. These budgets are often further supplemented in-year by additional national NHS or external funds secured through bidding processes.
Our Constitution, developed with the engagement of system partners and other stakeholders, sets out our purpose, powers, and governance and leadership arrangements to ensure the effective discharge of our duties and responsibilities.
Read our constitution and standing orders
Read the handbook to the NHS constitution
This explains each right and pledge in the NHS Constitution and the legal sources of both patient and staff rights and outlines the roles we all play in protecting and developing the NHS. These rights have been continued by the NHS South West London Integrated Care Board.
1.2.1. Our South West London Integrated Care System
NHS South West London was established on 1 July 2022 when we took on statutory status alongside the other 41 ICSs in the country. Building on the partnership work from previous years, NHS South West London has been working collaboratively with our partners to lead the development of our system including the development of neighbourhood health and care and the delivery of the three shifts in the 10 Year Health Plan.
1.2.1.1. South West London ICS: Provider Collaboratives
Our providers are working closely together to:
- reduce unwarranted variation in outcomes and access to services
- improve outcomes in population health, healthcare and tackling inequalities
- promote better quality care and best practice
- increase our resilience across systems – capacity, improving recruitment and retention
- achieve the benefits of working together at scale.
There are three provider collaboratives in South West London:
- South London Mental Health Partnership is made up of:
- South West London Acute Provider Collaborative is made up of:
- Royal Marsden Partners is made up of:
- all South West London and North West London organisations supporting the NHS cancer pathway, including primary, acute and specialist providers and screening services.
Our collaboratives have delivered significant achievements in the recovery of acute services following the pandemic, high quality cancer care and efficiency and high-quality care in Mental Health placements.
1.2.2. Leading our system and working in partnership across South West London
We are committed to a collaborative leadership approach for the benefit of local people across South West London. We have an experienced team of people working within our ICB, our partnerships and providers. Our role as an ICB, means that we lead the development of our system alongside our partners across South West London. Key areas in which we take on this leadership role, as well as our assurance function, include:
- Setting strategy – read more in section 1.2 About us
- Managing our money – including our system financial challenge – read more in section 1.3 Financial summary
- Improving performance – read more in section 1.5 Assuring delivery of performance
- Improving quality – read more in section 1.7 Improving quality and safety
- Addressing health inequalities and improving equality, diversity and inequalities – read more in section 1.16 Addressing health inequalities
- Socio economic development including the role of our partners as anchor institutes – read more in section 1.10.03 Our role as an anchor institution
We work with our partners and lead on the development of our key system strategies and plans.
As well as having strong governance and strategies in place, we work together across the system to ensure our services are efficient and high performing for the benefit of local people.
1.2.3. Integrated Care Partnership strategy
We developed our Integrated Care Partnership Strategy for 2023 to 2028 with our ICP partners and published this in July 2023.
Over the past eight years, our partnership has strengthened, and we have grown more confident in how we work together. However, like many systems across the country, we are operating in a more challenging financial environment and with local health and care needs continuing to grow, working differently is now more important than ever.
By collaborating at scale across South West London – when it is right to do so – we can focus our efforts and investment on the priorities that will make the greatest impact. Our Integrated Care Partnership Strategy explains how we have listened to one another’s challenges, reviewed data and evidence, and sought the views of local people across our six boroughs to shape how we tackle key issues together.
Our strategy, identifies six shared priorities:
- Tackling and reducing health inequalities
- Preventing ill-health, promote self-care and supporting people to manage their long-term conditions
- Supporting the health and care needs of children and young people
- Focusing on mental well-being
- Supporting older and frail people in the community
- Workforce
In addition, we have identified these areas of focus to embed in all our work:
- Equality, diversity and inclusion
- Championing the green agenda
- Elevating patient, carers and community voices
You can read the Integrated Care Partnership Strategy on our website.
1.2.4. National NHS direction and clustering arrangements
The national Model ICB Blueprint published in May 2025 set out the future role of ICBs as strategic commissioners, with a stronger focus on population health, neighbourhood services and reducing health inequalities. It also establishes a nationally set £19 per-person running cost for ICBs.
During 2025/26, NHS South East London ICB and NHS South West London ICB began to work more closely together to deliver the Model ICB Blueprint and the NHS 10-Year Health Plan.
Both organisations remain separate statutory organisations, with their own boards and legal responsibilities. There are no plans to merge. The two Boards agreed to enter a clustering arrangement. Under this arrangement, the ICBs share:
- a single Chair
- a single Chief Executive
- a single executive team
Place-based leadership arrangements in South West London remained unchanged.
This approach strengthens strategic commissioning capacity across south London, reduces duplication and improves organisational resilience, while maintaining local accountability.
During the year, Sir Richard Douglas was formally appointed Joint Chair for both ICBs and Andrew Bland was formally appointed as the shared Chief Executive for both organisations.
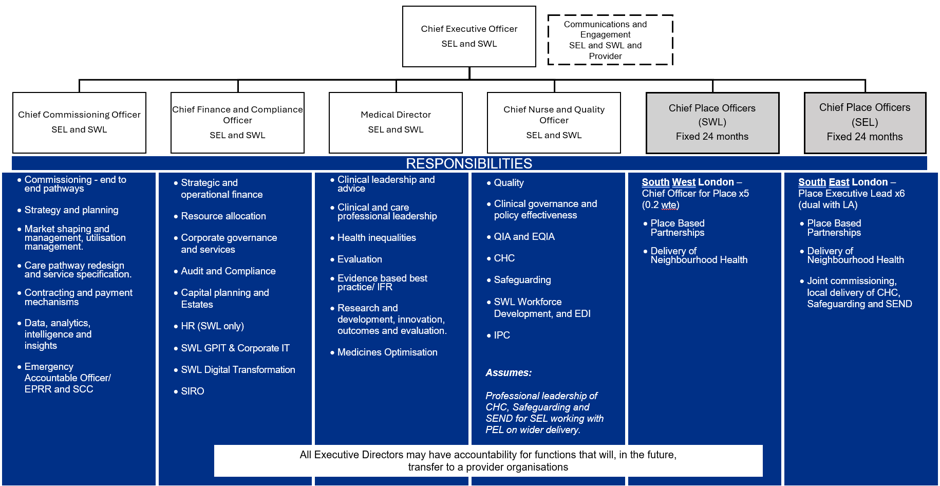
In March 2026, we launched staff consultation on a proposed structure for the organisation including some clustered teams. This builds on the new executive management structure that is outlined below. The staff consultation closed in April with a final structure shared with staff in May 2026.
1.2.5. The 10 Year Health Plan
In July 2025, the NHS 10-Year Health Plan was published. It sets out the long-term direction for the NHS and is centred on three shifts:
- From hospital to community
- From analogue to digital
- From sickness to prevention
The Plan confirms the role of Integrated Care Boards as strategic commissioners of local health services, with greater emphasis on neighbourhood health services, population health outcomes and financial sustainability.
In South West London, the priorities set out in the 10-Year Health Plan align with our existing focus on strengthening neighbourhood health, reducing health inequalities and supporting earlier intervention and prevention.
Through our commissioning plans and partnerships with local authorities and providers, we are embedding the three shifts into how services are designed and delivered. The Plan will continue to shape our priorities in the years ahead.
1.2.6. Neighbourhood health and care
A key part of the 10-Year Health plan is delivering, more care where people live.
In London, The Target Operating Model for London for Integrated Neighbourhood Health, published in May 2025, sets out how neighbourhood health will work in practice.
Neighbourhood health and care is already central to how services are organised in South West London.
Neighbourhood teams are led locally by partners working together around their communities. This includes general practice, community services, mental health services, hospitals, councils and voluntary organisations. How teams work reflects the people who live there, the services already in place, and what works best locally.
The ICB’s role is to set clear outcomes for neighbourhood health, agree plans with local partners and ensure public funding is used effectively. We align neighbourhood work to our wider strategy for South West London and provide system oversight, data and coordination to support deliver.
The ICB does not design or run local neighbourhood teams this remains at place level.
1.2.6.1. How accountability works
Neighbourhood plans are developed locally and agreed with the ICB. Over time, partners will identify a lead organisation to hold responsibility for delivery on behalf of the partnership, giving clarity without shifting delivery away from place.
1.2.6.2. What happens next
Local partnerships are developing neighbourhood plans for 2026/27. The ICB is putting the right framework and governance in place to support this work as it continues to develop.
Read more about the development of neighbourhood health and care in each of our boroughs in section 1.4 South West London Places.
1.2.7. Our local strategies
1.2.7.1. Our Joint Forward Plan
Our Joint Forward Plan describes how NHS partners across South West London are working together over the next five years to meet the needs of local people. The ambitions outlined in our plan are built from our understanding of the health needs of people in South West London, the health inequalities that exist and importantly the views, experiences and concerns of our people and communities.
There is no doubt that this is a challenging time for health and care services, but we are recovering well from the pandemic, and we will continue to work together to improve further. We are clear that achieving the ambitions in our Joint Forward Plan will need us all to work together differently, as we shift our focus from treatment to prevention, support people to make healthy choices, and improve our services and the way we provide care. We want to ensure that our ambitions are clear and respond to the needs of our patients, carers, residents and staff. We have developed our Joint Forward Plan for delivery throughout 2023 to 2028 which you can read more about on our website.
1.2.7.2. Strategic commissioning plan: transforming care together
Our five-year commissioning plan sets out the commissioning priorities for South West London ICB over the next five years to meet the needs of local people. The ambitions outlined in our plan are built from our understanding of the health needs of people in South West London, the health inequalities that exist and importantly the views, experiences and concerns of our people and communities and builds on our previously published Joint Forward Plans.
Our focus is to:
- Prevent ill health and support people to self-care
- Reduce health inequalities
- Keep people well and out of hospital
- Provide the best care wherever people are accessing our services
- Use technology to improve care
- Manage our money
- Make South West London a great place to work
- Deliver the NHS’ requirements of the Integrated Care Partnership Strategy.
Our priorities are to:
- Reduce the growth in prevalence and progression of ill health
- Transform models of care and reduce health inequalities
- Manage our money
- Improving productivity, efficiency and financial delivery in our Trusts
We are also developing a Clinically Led Strategic Plan to address system-wide challenges that require long-term transformation:
- Variation in quality, outcomes and widening health inequalities
- An ageing population with rising, complex needs
- Rising demand for healthcare
- A workforce under pressure
- Poor estates and infrastructure
- Significant financial challenge
This remains in development and once the ICB agrees the recommendations from our strategic plan will be reflected in our future Joint Forward Plan.
To determine our case for change we:
- Have reviewed the needs of our populations: analysing current and future health needs (further detail available on request) and feedback from our patients and population (a summary of this insight is below with further details in Appendix 1).
- Have agreed priorities for change and set up clinically led workstreams to redesign new models of care: building on success from SWL & elsewhere.
- Have set clear principles for redesign: prevention first, personalised care, equity of access, efficient & aligned capacity, integration, digital as enabler
You can read more about our performance against these standards in section 1.5 Assuring delivery of performance and constitutional standards.
1.2.8. Engaging clinical care professionals in our work
Clinicians and other healthcare professionals in NHS South West London have an essential role within our health and care system: as clinical leaders, those working with patients daily, those transforming care pathways, teaching a new generation of health and care professionals and pursuing research excellence.
In South West London, we work with local clinicians and other healthcare professionals to develop the right high-quality services for local people and to ensure clinical stewardship of the commissioning decisions being made. We support and resource clinicians and professionals from a variety of backgrounds to lead programmes of work and support the development of our cross-system strategies.
In 2024/25, we became a GMC training location for postgraduate public health medical training which enables us to host public health registrars, GP trainees and other specialities. We continued to host SPIN fellows (fellowship opportunities for newly qualified and early career GPs and General Practice Nurses and nurses new to practice, within one year of joining general practice) working on a range of projects including diabetes, developing multimorbidity approach to long term conditions and immunisations. We are committed to supporting clinical leadership and research, collaborating with our research and education leaders in our provider trusts, primary and community care and supporting the professional development of healthcare professionals.
In South West London we have nine clinical networks for areas of care: cardiology, ear, nose and throat services (ENT), gastroenterology, general surgery, gynaecology, ophthalmology, respiratory, trauma and orthopaedics and musculoskeletal and urology. Clinical networks enable patients, professionals and organisations to work together on large scale, long-term programmes of quality improvement.
1.3. Financial summary
NHS South West London is responsible for investing the funding we receive to maximise the health of the local population and overseeing the delivery of services by NHS organisations within the geography to both the South West London population and beyond. As both a system leader and commissioner we seek best value from our investments and have ensured effective use of funds through the Provider Selection Regime and the new Procurement Act 2023 requirements. To support the system financial position the ICB reviewed its investments in year and set itself a surplus target.
This section summarises the ICB’s annual accounts including the control’s assurance and auditor’s statements. Our performance against the key financial performance indicators is summarised below.
1.3.1. Finance summary
We received funding of £4.46 billion in 2025/26 and delivered a breakeven position as at 31 March 2026. This formed part of the wider draft South West London ICS financial position (breakeven after £103 million fixed cost support). We worked alongside the system to try and minimise any additional spend and maximise savings, whilst focussing on delivering high quality healthcare to as many people as possible.
For 2025/26, NHS South West London had an efficiency programme totalling £37.1million. During the year the ICB achieved an efficiency of £37.6 million, of which £31.4 million was recurrent and £6.2million non-recurrent.
NHS South West London is responsible for investing the funding we receive to maximise the health of the local population and overseeing the delivery of services by NHS organisations within the geography to both the South West London population and beyond.
Within the funding received there are certain requirements and conditions as to where and how these can be spent. The ICB ensured that we met all these requirements in year, with the key areas being:
- Ensuring we continue to increase our investment in mental health services called the mental health investment standard (an additional £43.4 million was spent in year)
- We remained within the £29.2 million running cost allocation for the ICB (excluding redundancy funding)
We also led the systemwide capital programme, working with providers to determine how annual system capital budgets are best utilised and ensuring delivery of key programmes of work. Further detail can be found in section 1.13 Capital investment.
1.3.2. How we spent our funding
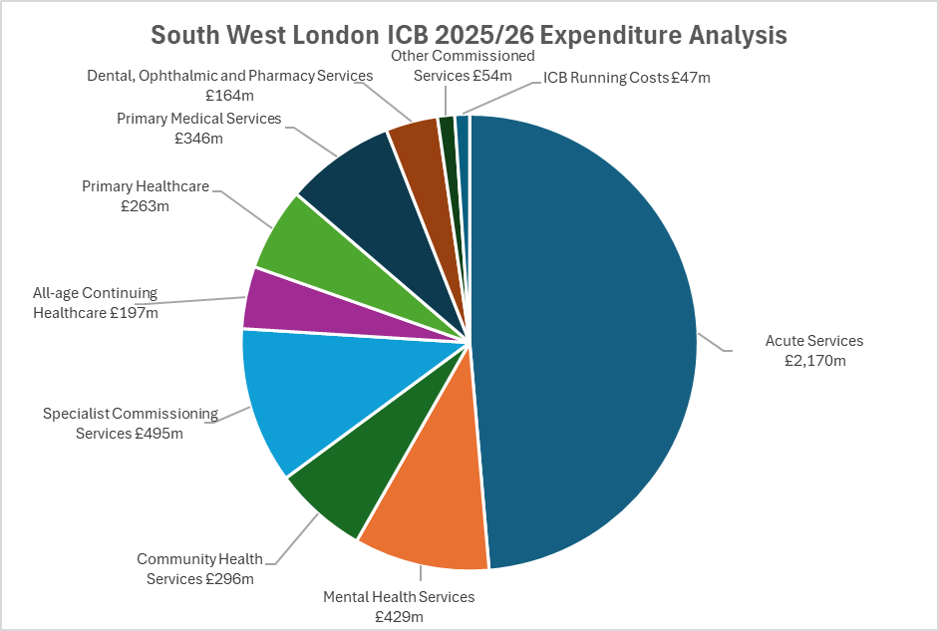
During 2025/26 the ICB spent £4,461 million.
An analysis of the ICB’s net expenditure by commissioned area in 2025/26 is set out below.
1.3.3. Mental Health Investment Standard (MHIS)
The table below details the ICBs Mental Health Investment Spending as a proportion of its programme allocation. Programme allocation excludes delegated primary care and running cost allocations.
| 2025-26 £’000 | 2024-25 £’000 | |
| Eligible Mental Health Expenditure | 363,376 | 319,700 |
| Total operating expenditure | 4,517,170 | 3,797,004 |
| Mental Health Expenditure as a proportion of total expenditure | 8.04% | 8.42% |
During 2025/26 the ICB was required to increase its Mental Health Investment Standard (MHIS) spending on specific services by 4.93% over the value spent in 2024/25. The MHIS spend for 2024/25 was £319.7m and therefore the target set for 2025/26 was £363.1m. The ICB spent £363.4m on MHIS services for 2025/26 and therefore achieved the target. The MHIS figure differs from the Mental Health services figures shown in the above pie chart as there are certain areas of spend that are included and excluded from MHIS spend as defined by NHS England’s MHIS guidance.
1.3.4. Financial governance and spending
We want to ensure we maximise value for money and invest our money to enable high quality services for our populations. Key to this is ensuring we continuously review our spend to ensure we are as efficient as possible. Part of this approach is our savings programme of £37.1 million, which we exceeded by £0.5m, with 83% of the savings being recurrent. We will build on this programme in 2026/27 to deliver further recurrent savings to ensure the maximum amount of funds are available for commissioning healthcare services.
While we don’t have to work to a specific threshold for agency spend, we ensured we had robust processes in place to review recruitment and minimise the need for high-cost posts, so the maximum level of funds went to direct healthcare. We will build on this programme in 2026/27 to deliver further recurrent savings to make sure the maximum amount of funds is available for commissioning healthcare services.
Further to this, we supported the wider system with identifying opportunities and sharing best practice to support the delivery of their organisational savings targets. This included providing oversight and analysis of spending patterns and performance against the agency threshold.
1.3.5. Financial governance and reporting
We have clear financial governance arrangements for managing spend during the year. These operated in accordance with guidance received from NHS England and Improvement, the ICB’s Standing Financial Instructions, Scheme of Delegation and Standing Orders.
In year we have continued to test and to strengthen our controls using various tools, as well as benchmarking them against other organisations across the ICS. Our financial policies are continuously reviewed to ensure they align with any new national requirements.
1.3.6. Going concern
The accounts have been prepared on a going concern basis. Public sector bodies are assumed to be going concerns where the continuation of the provision of a service in the future is anticipated, as evidenced by inclusion of financial provision for that service in published documents.
1.3.7. 2026/27 planning guidance and financial outlook
2026/27 is a year of change for the ICB as we deliver the functions as per the model ICB blueprint. The consequence of this is that we will no longer have a SWL control total and the ICB must develop a commissioning plan within its own resources and not linked to the other organisations within SWL.
We have developed a financial plan for 2026/27 which is a breakeven against the expected funding allocation. Whilst we are no longer tied to the financial delivery of our SWL partners we do have to be mindful of their financial resilience as they deliver services to our population. This makes delivering current services challenging and increases the requirement for efficiencies and improved productivity across all healthcare providers as we free up resources to enable the government ambition in the 10-year plan to move services out of acute and into community and primary care (“left shift”).
The new ICB will ensure that its governance structure is set up so that it has a focus on its strategic commissioning objectives, that value for money is being delivered and expected outcomes for patients is evidenced.
The focus of the work for 2026/27 is around ensuring the improvement in our planned care in line with national expectations, continued investment in mental health via the MHIS and transformational change with system partners to deliver the left shift as per the 10-year plan.
Our ICB ambition is to enable the redirection of funds into continuing to address health inequalities and preventing illness.
1.4. South West London Places
South West London is committed to working with local communities and neighbourhoods to make sure we respond to local health needs. Our places with delegated responsibilities, aligned to our six local authorities, and are an important part of our system. These six places work closely with NHS providers, local authorities, primary care, the voluntary sector and local communities to deliver on the key purposes of place:
- Support and develop primary care networks which join up primary and community services across local neighbourhoods
- Simplify, modernise and join-up health and care including through technology and by joining up primary and secondary care where appropriate
- Understand and identify – using population health management techniques and other intelligence – people and families at risk of being left behind and to organise proactive support for them
- Coordinate the local contribution to health, social and economic development to prevent future risks to ill-health within different population groups
1.4.1. Our role in delivering health and wellbeing strategies
We are committed to working with our local Health and Wellbeing Boards to develop plans that support the health and wellbeing of our residents. Across each of our place partnerships, we have developed Health and Care Plans that support the delivery of each borough’s Joint Health and Wellbeing Strategy. These strategies are developed by the Health and Wellbeing Board, to meet the health needs identified in the borough’s Joint Strategic Needs Assessment (JSNA). Each of our Place leads for Health represent their place on the local authority Health and Wellbeing Board along with representatives from local NHS acute, mental health and community providers, Healthwatch, community and voluntary sector and other partner organisations.
Read the Health and Care plans for each place on our website
You can find details of each borough’s Health and Wellbeing Board on the local authority websites:
1.4.2. Our place-based partnerships
We have a strong history of partnerships at place level, and these continue to grow each year. Our place-based partnerships lead the detailed design and delivery of integrated services across our local communities and neighbourhoods.
Our place partnerships involve the NHS, local councils, community and voluntary organisations, residents, people who use services, their carers and representatives and other community partners with a role in supporting the health and wellbeing of the local population.
We have been developing ways of working with our partners at place including local authorities, NHS provider trusts, Healthwatches and voluntary and community sector. We have examples of place partnership below, that show the delivery of borough health and wellbeing strategies and health and care plans.
Content for our place elements has been shared with our six Health and Wellbeing Boards.
1.4.3. Croydon
Croydon is the largest of our South West London boroughs and the largest London borough overall by population. It includes Coulsdon, Purley, South Norwood, Norbury, New Addington and Thornton Heath. Croydon is also the South West London borough with the widest health inequalities, these are unfair differences in health and health outcomes. 50% of the most deprived South West London residents live in Croydon and 40% of residents who are most likely to have physical and mental health conditions. With 52% of the population being from Global Majority, Croydon is also the most ethnically diverse local authority within South West London. The local NHS, Croydon Council, Voluntary and Community Sector (VCS) partners collaborate as the ‘One Croydon Alliance’ to meet the health and care needs of local people. During this year the Alliance made progress in making improvements for residents including Frontrunner, Integrated Neighbourhood Teams and Health Communities Together.
1.4.3.1. Locally Commissioned Schemes
Following a formal evaluation of Croydon PMS premium services and Locally Commissioned Services (LCS) in primary care in 2024/5, these were reviewed throughout 2025/6 to assess for value for money, impact against population health and strategic priorities
With engagement from both primary and secondary care colleagues, the review looked at either amending or terminating existing schemes and explored opportunities to re-invest in new schemes to ensure that our resource was aligned with the NHS 10-Year plan and address the health inequalities we continue to see in Croydon.
The review resulted in a transformation to the way we delivered enhanced services for General Practice and we worked closely with practice manager colleague so that we co-designed solutions together. The completion and agreement of all service specifications were agreed by the LCS/PMS steering group, including the Local Medical Committee, with clear funding and reporting requirements. The revised and new specifications aim to deliver better value for money, support the NHS 10-Year plan ambitions (to shift activity from hospital to community and treatment to prevention), demand management of acute services, data driven commissioning and transformation while delivering optimal outcomes and a better experience for patients. Partners have worked together to mobilise the delivery of the new specifications which will begin seamlessly from April 2026.
1.4.3.2. New Addington Community Diagnostic Centre
In October 2025, we opened a new Community Diagnostic Centre (CDC) in New Addington. The state-of-art facility acts as a one stop shop and is located near to the main shopping parade in an area of long-standing health inequalities. The Centre is providing access to essential diagnostic tests and services including respiratory care, CT scans, cardiac ultrasounds, blood pressure tests and ECGs.
The CDC has provided specialist advice on diagnosis, reduced the length of time patients are waiting for care following a referral and simplified pathways for people who go on to need treatment. Since opening in November 2025, staff at the centre have seen 1396 patients for CT scans and 4280 ultrasound scans and the flexible staffing model has allowed us to pivot demand trends and ensured we are on track with the national DM01 target in Croydon. The walk-in x-ray service is growing in popularity as more in the community become aware of the provision and has seen 672 patients since November.
The CDC also offers opportunity for community-based support and allows us to expand primary care access with a local GP offering additional GP appointments in the building from April 2026.
1.4.3.3. National Neighbourhood Health Implementation Programme
With the NHS 10 Year Plan aiming to transform the way care is delivered to person-centred support delivered through neighbourhood teams, Croydon was selected this year as one of 43 first wave of areas across England to pilot the National Neighbourhood Health Implementation Programme.
Working as the One Croydon Alliance since 2017, NHS organisations have worked in partnership with the local authority and voluntary and community organisations to join up health and care through Integrated Neighbourhood Teams. The national pilot is accelerating progress to test improved ways of working to get the best possible outcomes.
An initial workshop in October 2025 was attended by over 70 partners where we looked at which groups would benefit most from this new way of working and which models we wanted to test. We agreed that the pilot would look at adults with more than one long-term condition, initially focusing on people who are at risk of poor care coordination but are not yet high users of unplanned hospital care.
Three Croydon GP practices (one in the north of the borough, one in the centre and one in the south), tested some new approaches. This involved more senior clinicians and managers being part of the multi-disciplinary team ‘huddle’ at the Practice, better integration of mental health support and joint consultations or visits with more than one practitioner, rather than multiple appointments for the resident to attend.
Learning from the pilot will inform improved ways of working across the whole of Croydon and will help shape how neighbourhood health is implemented across South West London and beyond to the rest of the country.
1.4.4. Merton
Merton includes Wimbledon, Mitcham, Morden, Raynes Park, Colliers Wood, Wimbledon Park, South Wimbledon and Eastfields. The gap in life expectancy between the 10% most deprived and the 10% least deprived in Merton is 7.7 years for men and five years for women. Of the 340,000 population in South West London that have the most health needs, 29,000 are located in East Merton.
Health and care organisations in Merton work together to reduce inequalities and provide truly joined-up health and care services with and for all residents, so they start, live and age well in a healthy place. During this year a range of activities and initiatives have had a positive impact on the health and wellbeing of local people.
1.4.4.1. Improving respiratory health in Merton
In Merton, our GP Federation (Merton Health CIC) with support of the Health Innovation Network South London, was awarded funding from the NHS England Respiratory Pathway Transformation Fund for a six-month pilot which ran from 1 October 2025 to 31 March 2026. As one of ten areas across England, partners across health, social care and the voluntary sector worked together to improve respiratory health during the winter.
Based in clinics local to residents’ homes, the pilot has improved access to high-quality respiratory diagnostics delivered through GPs alongside specialist respiratory input provided by Central London Community Healthcare NHS Trust and the St George’s, Epsom and St Hellier Hospital Group. The proactive and preventative approach targets reviews for patients at highest risk of worsening outcome and allows clinicians to better support patients to manage their own conditions, reduce avoidable admissions and improve quality of life.
Across Merton more than 500 residents with respiratory conditions were supported by the pilot which aimed to support earlier detection of chronic obstructive pulmonary disease (COPD) and strengthen proactive care and support for those with COPD and asthma. The success of the pilot has led to the funding being extended into 2026/7.
1.4.4.2. Holistic Assessment and Rapid Investigation (HARI service
The Holistic Assessment and Rapid Investigation (HARI) service is a unique initiative available to Merton residents to help prevent hospital admissions, reduce risks of falls and enable independent living. The service is funded via the Better Care Fund and is located within the Nelson Health Centre. The initiative can only be accessed on site however transport is offered for anyone who is unable to travel independently.
HARI is an opportunity for Merton residents living with multiple long terms conditions to visit the Nelson Health Centre and see a number of professionals in one visit. During their visit, patients can receive diagnostics and be prescribed information, support and interventions to help with their health and wellbeing.
The team is made up of a range of professionals such as physiotherapists, occupational therapists, advanced nurse practitioners, pharmacists and also a St George’s geriatrician. The site has a model kitchen and bathroom which enables patients to work with the team to show their capabilities within a ‘home environment’ and work together on ways to manage everyday tasks and live independently. The initiative also features regular rehab classes for residents who have recently recovered from a fall – these classes are a great social opportunity particularly for residents who may live alone. There has been on average around 35 referrals a month for the HARI service with one average 82 patients on the caseload per month. This year we have tested an urgent 48-hour pathway from St George’s Hospital into HARI. We are still working to maximise the opportunity of this urgent pathway, but the groundwork has helped to strengthen relations between the community and acute provider.
1.4.4.3. Speech and Language Therapy Service
In Merton, we are working with Merton Local Authority and Central London Community Health Speech and Language Services to align practice across the services to better support children and young people with communication needs. This will ensure that children receive the right support and the right time and place.
1.4.4.4. Merton Primary Care
The 21 GP practices in Merton deliver a wide range of services to their patients at practice, PCN and borough level. This includes a range of diagnostics, meaning patients do not have to attend a hospital setting. Over the last year practices have delivered over 52,000 phlebotomy tests and 1,000 24 hours Ambulatory blood pressure monitoring
Practices also have a focus on delivering proactive care to their most vulnerable patients, including those at End of Life, identifying those who would most benefit from the holistic assessment, care planning and MDT approach, with over 1500 patients managed in this way, plus an additional 700 patients in care home also benefiting. The MDTs include professionals from the primary care, community services, local authority and the voluntary sector, to support patients to remain at home, and receive the right care at the right time.
Access to primary care is available 8am-8pm seven days a week through a combination of practices, PCN access clinics and two boroughwide access hubs at Wide Way Medical Centre and The Nelson Health Centre, altogether offering in excess of 89,000 appointments a month. All practices now offer total triage for their patients to support access to more timely care, and are embracing new digital ways of working, whilst also ensuring that all patients are still able to access the practice even if they do not want to use or unable to use the digital offer. Recent work with SGH has also enabled the Emergency Department to book patients directly into GP appointments at the access hubs, enabling patients to be redirected to a more appropriate setting. This builds on the ability of NHS 111 to book patients in these hub appointments.
1.4.5. Kingston and Richmond
1.4.5.1. Kingston
As well as Kingston upon Thames, the borough includes Surbiton, Chessington, Malden Rushett, New Malden and Tolworth. There is a six-year gap in life expectancy between the most and least deprived men, and a four-year gap for women with the gap widening over the last decade. The number of people over 65 is above the London average at 14.4% of the total population and the number of people over the age of 80 is set to grow by 37% in ten years.
Local NHS organisations, the council and voluntary and community services in the borough are working together towards goals set out in its health and care plan, in partnership with local communities. This year the partnership delivered a range of programmes to deliver its aims.
1.4.5.2. Richmond
Improving health and wellbeing in Richmond, including Barnes, East Sheen, Mortlake, Twickenham, Teddington and Hampton. The number of people over 65 is above the London and national average at 16.2% of the total population and 19,604 (36%) people have more than one long term condition. There are also an estimated 4,600 children aged 5-19 years old with a diagnosable mental health disorder.
The Richmond Place health and care partnership works together to improve the health and wellbeing of children, young people, adults and older people. During this year the partnership achieved a lot through working together.
1.4.5.3. Children and young people mental health
Mental health support for children and young people continues to be a focus across Kingston and Richmond this year – improving access, reducing waiting times and creating more consistent pathways of care. Our CAMHS service is now being delivered by a single provider, South West London and St George’s Mental Health Trust, which was one of the key recommendations from an independent review into long waits and high levels of need, including the highest admissions for self-harm in London.
With the transfer completed from Achieving for Children to the Trust, staff are now embedded across local sites and records and waiting lists have been fully transferred, ensuring continuity of care. The focus is on reducing waiting times, to support children and young people to be seen in a timely way.
Alongside this, we are taking action to reduce emotionally related school avoidance through a more coordinated local pathway and continuing to expand the reach of Mental Health Support Teams, who are supporting schools with rising levels of anxiety, low mood, and behavioural needs.
1.4.5.4. Neighbourhood Health and Care
Across Kingston and Richmond, our neighbourhood health and care work is focused on clear, practical actions that will help us to improve prevention, support earlier intervention, and reduce inequalities. Over the last year, we have brought partners together to agree shared priorities across the life course, and this includes a plan to launch a family proactive care model to give families earlier, more coordinated support, building on our Family Hubs in both boroughs; reducing cardiovascular risk, through primary and secondary prevention; improving mental wellbeing and resilience of residents; and continuing to deliver our frailty programme to help older people stay independent for longer.
Underpinning the delivery of our shared neighbourhood priorities are three key principles: embed carers’ voices, resident insight, and fairness of access in everything we do. We will use population health data, enhanced neighbourhood digital tools, and the Pro-active Anticipatory Care (PAC) model to deliver more joined up support. Our partnership working across Kingston & Richmond was recognised at the London Personalised Care Awards when the service received the Collaborative Working Award, for contributions to supporting personalised care through the PAC model.
In the months ahead, we will be finalising our delivery plans, to develop neighbourhood programmes across Kingston and Richmond aligning to national guidance.
1.4.5.5. Frailty
We are strengthening our approach to frailty across Kingston and Richmond through our participation in the NHS England National Frailty Discovery Collaborative, one of only seven areas selected nationally for our strong proactive care model, effective use of data and close partnership working across health, social care, and the voluntary sector. Together, we are designing and testing new ways of supporting people to stay independent and well at home, reducing unnecessary hospital stays and improving outcomes for our growing population of older residents.
As part of the national frailty work, Kingston and Richmond are leading on a national digital frailty pilot that will explore how health and care information systems can be better integrated, to empower patients and to support care providers to deliver an improved frailty service for our communities.
The project which launched on 1 December has a focus on:
- Improving the flow of patient information between GPs, hospitals, community services, social care, and voluntary organisations
- Using data to identify patients who need extra support before problems arise
- Testing more efficient ways of working
Insights from this pilot will help shape future policy and be shared with other NHS systems.
To meet rising levels of frailty among people aged 65 and over, we are developing a single, integrated frailty model that offers a consistent and patient centred pathway across both boroughs. Under the leadership of our Frailty Programme Board, the model aligns with the South West London Framework and focuses on strengthening prevention, delivering a holistic falls and frailty service, and improving support for care homes, rehabilitation, and multidisciplinary care. We are also expanding support for carers, enhancing frailty and end of life care for people with both cancer and non cancer conditions, and investing in education and training to equip our workforce with the skills needed to deliver high quality frailty care.
1.4.5.6. Kingston and Richmond virtual ward
The Kingston and Richmond virtual ward provides safe, hospital level care, with consultant level oversight for patients in their own homes. It has been very successful in supporting older people, reducing hospital admissions and readmissions, improving patient experience, and preventing hospital acquired complications. This year, we have focused on combining our step up and step down services into a single integrated model, expanding the range of conditions we can safely manage at home to include COPD and heart failure, strengthening GP engagement, and addressing digital exclusion by providing training and equipment to ensure all patients can benefit.
Our step-down pathway helps people leave hospital sooner with continued monitoring, testing, and treatment at home, while our step-up pathway supports those who become unwell suddenly, helping to avoid unnecessary admissions. Using remote monitoring technology tailored to each patient’s needs, we track vital signs and maintain regular clinical contact to provide effective, personalised care.
1.4.6. Sutton
Sutton includes Beddington, Belmont, Carshalton, Cheam, Hackbridge, St Helier, Rosehill, Wallington and Worcester Park. Sutton is within the top 10% most densely populated of all local authorities in England. The population has grown by 7% in the ten years to 2023, and 18% (38,500) of Sutton residents are in the Core20 or most deprived population in South West London.
Health and care partners in Sutton have a shared vision and principles to deliver preventative, proactive and reactive health and care – at the same time as supporting local people to play an active role in maintaining their own wellbeing as a community. This year the partnership has delivered a range of initiatives and interventions.
1.4.6.1. Neighbourhood health and care: delivering priorities closer to home
This year, partners across Sutton continued to build on a neighbourhood health and care approach, with a focus on better coordinating services for residents with the highest levels of need. This includes people living in care homes, residents who are frail, those who are housebound, and people approaching the end of life. Neighbourhood working brings health, social care and community partners together around local populations, helping to provide support earlier and in a more joined-up way. Through neighbourhood working, partners have focused on the following priority areas: preventing cardiovascular disease (CVD) through neighbourhood working; proactive care for people with complex needs; and supporting timely hospital discharge and independent living at home. For CVD for example, neighbourhood working supports earlier identification of people at risk and more timely and tailored support. By strengthening links between primary care, community services and local prevention offers, neighbourhood teams are helping residents to access support that promotes healthier lifestyles and reduces the risk of CVD over time. This also helps to reduce longer-term pressure on health services.
1.4.6.2. Improving access and experiences for families navigating SEND services
Services for children and young people with Special Educational Needs and Disabilities (SEND) continue to face significant pressure locally and nationally. Partners across health, care and education in Sutton have focused on improving how families experience support by working more closely together. A key priority has been making support clearer, more timely and easier to access, helping to reduce fragmentation between services. This includes strengthening the local offer so families have better information about the full range of support available locally. Partners are also testing a more needs-based approach, particularly for children and young people with neurodevelopmental needs, enabling families to access appropriate support earlier and without unnecessary delays. Alongside this, work is underway to improve access to children’s therapies which includes reviewing therapy provision for younger children and developing simpler information for families about how to access therapy services. By strengthening collaboration across health, care, education and community services, this work aims to improve family experience, support earlier intervention and ensure support is shaped around children and young people’s needs.
1.4.6.3. Support for people with learning disabilities
Organisations across Sutton have continued partnership work this year to improve the health, wellbeing and independence of people with a learning disability. Our aim is to build an inclusive and supportive borough where people with learning disabilities and their families are empowered and valued. Through Sutton’s Joint Learning Disability Strategy we set out our commitments to improve annual health checks, increase meaningful employment and support residents to live the place they call home. Through the Better Care Fund planning process for 2025/26, we have identified additional resources to enable an expansion of the Sutton independent living offer. This has included changes to a small number of specific music and drama therapy sessions while a comprehensive mental health and wellbeing support service remains in place.
1.4.7. Wandsworth
This inner London borough includes Battersea, Tooting, Putney, Balham, Roehampton, Furzedown and Southfields. It has the second largest population in inner London with 327,506 residents. Wandsworth has one of the youngest populations in the country as well as one of the fastest rates of population growth in London. Half of the adult population is classified as overweight or obese.
1.4.7.1. Health and Care Partnership
The Wandsworth Joint Local Health and Wellbeing Strategy was published in 2024 and partners have worked together to embed and drive meaningful change across the partnership through the Wandsworth Health and Care Partnership. The partnership approach looks for opportunities for staff and residents to contribute to the delivery of the strategy, what factors could impact the programme, how to build in resilience and sharing best practice.
Wandsworth Health and Care Partnership brings together professionals from across the system including acute, community, mental health, primary care, adult social care, children’s services and colleagues from the voluntary and community sector. We use an integrated governance approach with rotating chairs to align to the life course of our shared strategy:
- Start Well – chaired by Wandsworth’s Director of Children’s Services
- Live Well – chaired by the ICB’s Director of Integration and a Local Authority Consultant in Public Health
- and Age Well – Chaired by a Chief Executive Officer of the VCSE
Each of the monthly meetings focuses on one of the life-courses and priority leads present progress, highlight challenges and seek support to remove barriers. Each meeting includes time to showcase initiatives addressing inequalities and amplifying the voices of seldom heard communities. The approach reduces duplication, improves collaboration and supports better health and wellbeing outcomes for all residents of Wandsworth.
This integrated approach, supported by an integrated governance framework has significantly increased the impact of interventions and delivered measurable outcomes for communities, particularly those at greatest risk of health inequalities. For example, our uptake of childhood immunisations has improved to 88% against the London average of 82%, referrals to our diabetes service increased from 890 in 2024 to 1,318 in 2025 and our dementia diagnosis rate reached 77.7% exceeding the national average of 66.1%.
1.4.7.2. Wandsworth Partnership for Inclusion of Neurodiversity in Schools
The Partnerships for Inclusion of Neurodiversity in Schools, PINS, programme is a national initiative aimed at supporting neurodivergent children in mainstream primary schools. It focuses on creating a supportive learning environment and improving the overall quality of education for neurodivergent pupils. The programme is designed to be needs-led, meaning it supports the needs of all children within a school setting, including those without a formal diagnosis. The initiative is part of the Government’s broader ambition to break down barriers to opportunity and ensure every child can achieve and thrive through an inclusive approach to Special Educational Needs and Disabilities (SEND).
In Wandsworth, the programme aims to provide a supportive learning environment for neurodivergent children, helping them develop the knowledge and skills they need to thrive as they grow.
The programme has now been rolled out across 16 of Wandsworth’s primary schools. Schools have been able to access webinars covering a wide range of topics co-designed with parents and carers to help neurodiversity including ‘understanding children’s behaviour’, ‘supporting communication’ and ‘understanding masking’. School staff and parents have also been able to access professional coaching through services such as Speech and Language Therapists, Occupational Therapists and Educational Psychology. Learning from this project will be embedded in our response to the government’s white paper on SEND.
1.4.7.3. Wandsworth – South Asian Cancer Screening
To improve uptake of cervical screening in Wandsworth, where coverage is as low as 44.3% in some communities, we have worked to raise awareness with a focus on increasing uptake among the South Asian community. Working as a partnership, the ICB, local authority’s public health team, voluntary sector, GPs, community services and RM Partners have worked to understand the reasons behind low uptake using behavioural insights and working with the community to co-produce meaningful, community-led solutions. Underpinned by principles of listening, building trust, responding and empowering the community to learn at their own pace we have delivered five community events delivered in English, Hindi and Urdu with local community groups including Happy Homes, Women of Wandsworth and Mushkil Aasaan.
Community members directly shaped the design, language and format of resources which include a leaflet, written and audio FAQs and an information video, which will be formally launched in April. These will shared by community groups and WhatsApp groups, local health settings and by social prescribers to help women to make confident choices about screening.
Since the work started, cervical screening uptake among the target communities has increased by almost 10% and survey data shows that women feel more confident discussing screening with family members and healthcare professionals.
1.4.7.4. Wandsworth Place Provider Alliance and Neighbourhood Health Services
Established on 1 April 2025, the Wandsworth Place Provider Alliance—comprising Central London Community Healthcare NHS Trust, St George’s University Hospitals NHS Foundation Trust, South West London and St George’s Mental Health NHS Trust, Wandsworth Care Alliance (VCFSE), Wandsworth Council, and Wandsworth GP Federation—brings partners together to improve population health and healthcare. As the delivery vehicle for the NHS 10 year plan, the Alliance has developed four neighbourhoods built around recognisable communities: Balham, Tooting & Furzedown; Battersea; Earlsfield, Southfields & Central Wandsworth; and Putney & Roehampton.
Neighbourhoods are already working differently—through deeper integration and partnership—to combine high quality Proactive Care (anticipatory care planning) with alternative care pathways via Urgent Community Response (rapid, home based intervention) and Virtual Ward services (multidisciplinary care and remote monitoring at home). This model ensures people living with frailty have robust care plans to keep them well and out of hospital, strengthening admission avoidance, same day response, and safe discharge to improve non elective (unplanned) performance. Multi agency leadership teams are in place to drive delivery against the South West London Clinically Led Strategic Plan.
Neighbourhoods also prioritise primary prevention and the needs of children and young people, addressing local determinants of health. In Battersea, for example, links with the Battersea Alliance support community development initiatives such as promoting the London Living Wage, alongside programmes that build resilience and improve uptake of preventive services.
Collectively, the Alliance and neighbourhoods are enabling the system’s shift from acute to community, analogue to digital, and treatment to prevention. As we move into 2026/27, this work will be critical to transferring resources into neighbourhood settings, truly bringing care closer to home and supporting South West London to mature as a strategic commissioner focused on securing the best services and outcomes.
1.5. Assuring delivery of performance and constitutional standards
NHS England assesses the performance of each ICB through a large number of national metrics. The performance measures (below) represent a cross section within the 2025/26 priorities and operational planning guidance.
These measures help us to monitor and improve the time patients have to wait to access services in South West London. They also tell us where we need to work with our partners to improve the care that our patients receive.
1.5.1. Elective
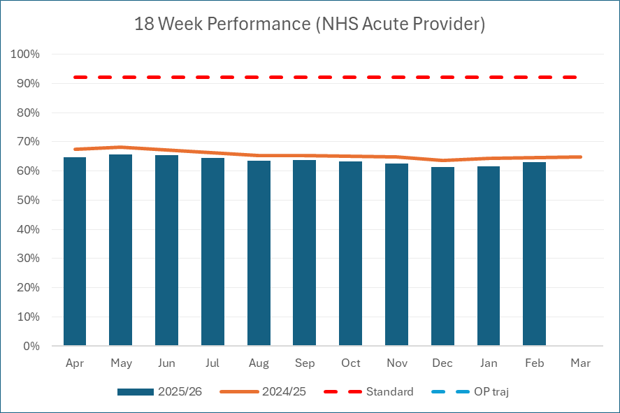
1.5.1.1. Referral to treatment
The NHS Constitution gives patients the right to have their non-urgent, consultant-led treatment start within 18 weeks of a referral. The proportion of patients waiting less than 18 weeks was 63.1% in February 2026 against a plan to achieve 65.8% by the end of March. Further improvements are expected before the end of the year due to a national performance sprint which saw additional national funding made available to NHS providers. Each provider agreed their own revised trajectories which demonstrated a clear improvement on their performance at December 2025.
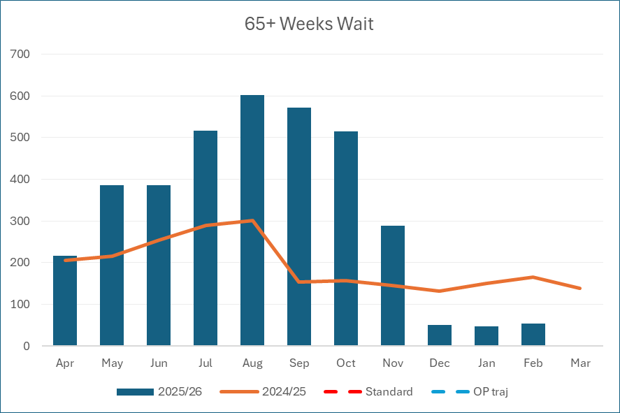
Following the unprecedented increase in people waiting for treatment after the Covid-19 pandemic, a national priority has been to reduce the longest waiting patients. This was measured by ICBs working to a trajectory to reduce the number of patients waiting over 65 and 52 weeks.
By February 2026, South West London hospitals had 54 patients waiting above 65 weeks, showing a marked reduction since the start of the financial year. This represents a reduction from a maximum of 600 in August 2025.
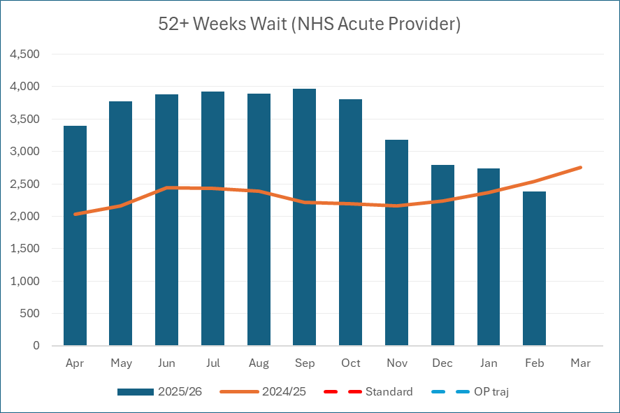
For 52 week waits, these levels have somewhat improved with 2,382 at the end of February 2026, compared to 3,392 at the start of the financial year, April 2025. SWL ICB had the lowest 52 week waits in London for February 2026 and we continue to work with our partners to further reduce waiting times. This work includes improving our productivity by sharing capacity across NHS hospitals, undertaking initiatives to improve services and reducing inequalities of access, supported by of our Clinical Networks and using independent sector provider capacity, where necessary.
1.5.1.2. Diagnostic test waiting times
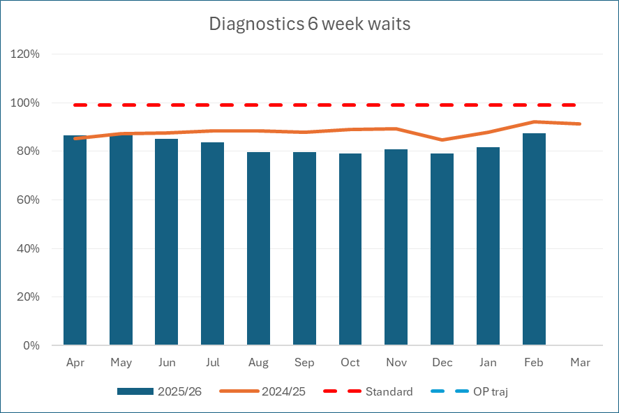
Timely access to diagnostic services is essential to support the 18-week referral to treatment pathway. This measure looks at the proportion of patients waiting for a test within fifteen key diagnostic areas. ICBs were given a target to ensure 85% of patients receiving these tests wait less than six weeks. The national standard prior to COVID was to ensure diagnostic tests were carried out within 6 weeks, in 99% of cases.
We have made some progress towards this goal by delivering more diagnostic tests than in the financial year 2019/20, before the impact of Covid-19.
Our performance has remained further challenged this year in comparison to 2024/2045, with the most recent month February 2026 at 87.4%, on track to meet our March target.
1.5.2. Urgent and emergency care
1.5.2.1. Accident & Emergency (A&E) four-hour performance (all type)
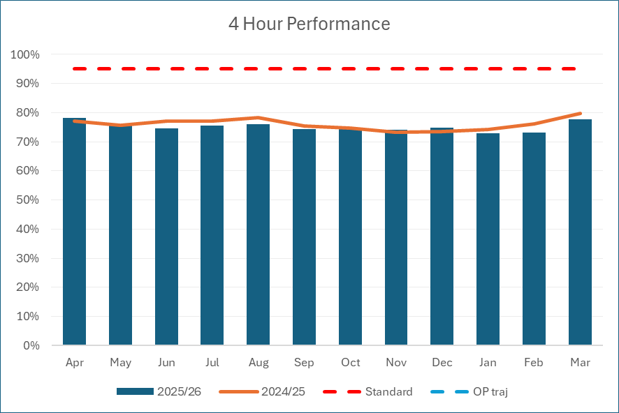
A&E waiting times are important for both better clinical outcomes and patient experience. One of the government pledges is that no patient should wait longer than four hours in A&E from arrival to admission, transfer or discharge. In 2025/26, the national plan was to ensure that a minimum of 78% patients arriving in A&E were seen in four hours by March 2026.
Our performance against the four-hour target has remained relatively consistent since April 2025. Recent data for, March 2026, shows that we achieved 77.8%, 0.2% short of our goal.
We have programmes of work in place for preventing unnecessary admissions and improving internal processes, which expedite safe discharge from wards to make the best use of resources. We have invested in a range of initiatives in coordination with A&E departments to appropriately reduce demand where patients can access the services they need without attending the emergency department. These include frailty services at the front-door, additional therapy and pharmacy services.
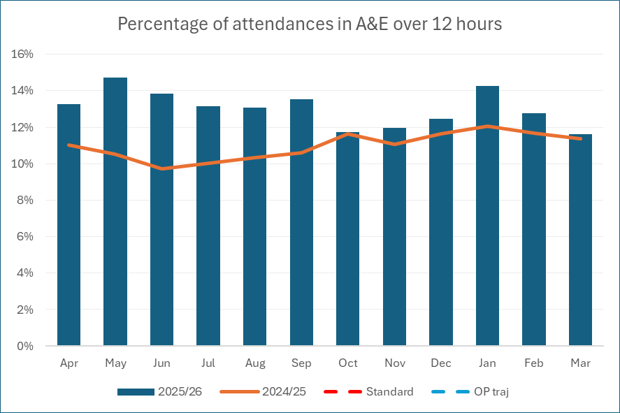
1.5.2.2. 12-hour breaches
The number of patients waiting over 12 hours in A&E from arrival has been comparatively high since April 2025. SWL ICB are currently in the lowest quartile nationally. In response we launched a two-year plan to improve Urgent and Emergency Care (UEC) services in the system.
Core workstreams within this plan sought to address themes around access, workforce, discharge and flow through the hospital. Improvements in each of these areas were overseen by the SWL UEC Board. In addition to physical health, a South West London Mental Health Improvement Plan is in place. This focussed on improving the pathway for patients presenting with mental health crisis at A&E and reducing delayed transfers of care through schemes such as step-down hostel capacity. The new virtual Section 136 hub has been implemented and is showing benefits with fewer patients needing an ambulance. Work is ongoing to address delayed transfers of care.
1.5.3. Cancer waiting times
The timely diagnosis and treatment of cancer is vital to support improved outcomes for patients.
As well as working towards earlier diagnosis of cancers by 2028, there were two cancer waiting time standards which were prioritised, nationally, for 2025/26. These were:
- 28-day faster diagnosis standard (77% standard)- patients should be diagnosed with a cancer or benign diagnosis withing 28 days of referral.
- 62 days referral to treatment (85% standard) – patients should start cancer treatment within 62-days from referral.
We have delivered strong performance against the cancer waiting times standards in South West London compared to the rest of London and England.
We continue to work in partnership with RM Partners (the West London Cancer Alliance) which includes NHS acute providers, community services, primary care, commissioners, public health and the voluntary sector to maintain and improve access to cancer services across South West London.
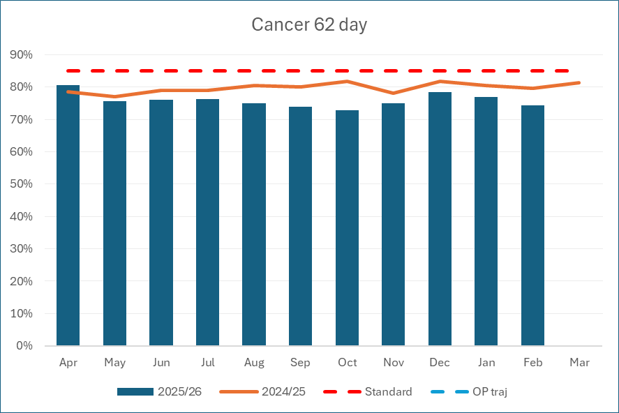
1.5.3.1. Cancer 62-day GP referral (Commissioner)
We were the second highest performing ICB in London against the 62-day performance standard for February 2026 with an outcome of 74.4%.
Although this was below the national standard of 85%, this was above the National average of 68.6% and London average of 69.4%.
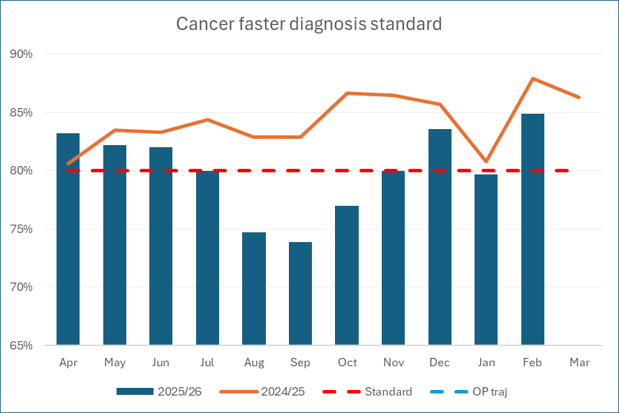
1.5.3.2. Cancer 28 day faster diagnosis standard (Commissioner)
Our Faster Diagnosis Standard performance for February 2026 was 84.9%. SWL was the highest performing ICB in London and performance above the National average of 80.5%. Performance outcomes were above the 77% target by all of the South West London providers.
1.5.4. Mental health and learning disabilities
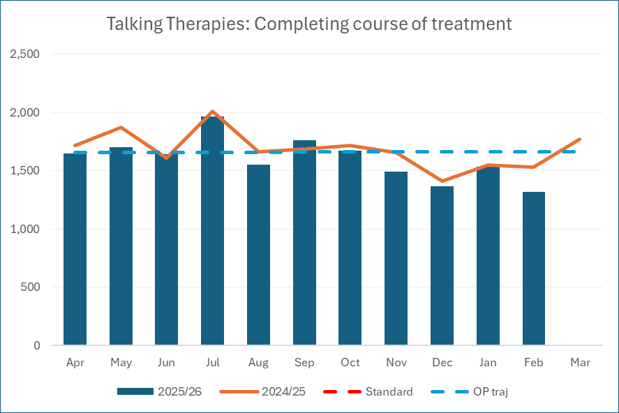
1.5.4.1. Talking therapies – Number of completed treatments
Around one in six adults in England suffer from a common mental health problem like depression or an anxiety disorder. NHS Talking Therapies provide evidence based psychological interventions for adults.
This metric replaced the count of new appointments starting in talking therapy services within the national operating plan requirement for 2025/26. The purpose of this count is to ensure sufficient numbers of treatments are being completed and that they are consistent with annual plans for maintaining recovery rates for our population.
SWL ICB has been above the annual plan since July 2025 until December 2025. December/January tends to see fewer treatments occurring due to the bank holidays and staff and patients on leave during these periods.
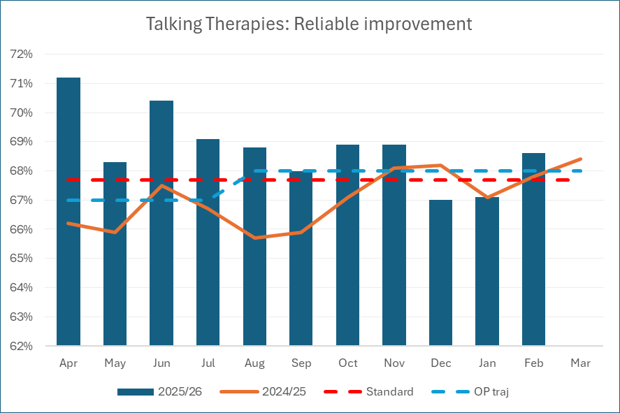
1.5.4.2. Talking therapies – Reliable improvement and recovery
Two other key metrics are reliable improvement and reliable recovery rate. Reliable improvement is where a patient has experienced a reduction in their anxiety and/or depression beyond a specified measure, during treatment, but may not have reduced below the ‘clinical threshold’ to conclude treatment. Reliable recovery is where an improvement meets both the defined amount deemed ‘reliable’ and reduces below a clinical threshold. Both are measures of the effectiveness of talking therapies.
The latest year-to-date position shows that 48.4% of people finishing a course of treatment experienced reliable recovery, as an average from April to February. This is just below the 48.6% national standard. Reliable improvement was 69.1%, as an average from April to February, against a 67.7% national standard.
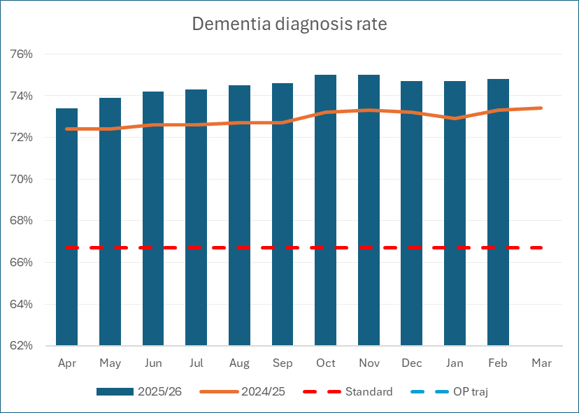
1.5.4.3. Dementia
A timely diagnosis enables people living with dementia, along with their carers and families, access treatment and support. This enables them to plan in advance how best to manage the impact of the condition; working together with professionals in primary and secondary care services to deliver personalised care plans.
In 2025/26 we maintained a performance level above the national threshold and were one of the highest performing ICBs in the country. February 2026 saw 74.8% of patients with dementia identified, compared to the 66.7% national target.
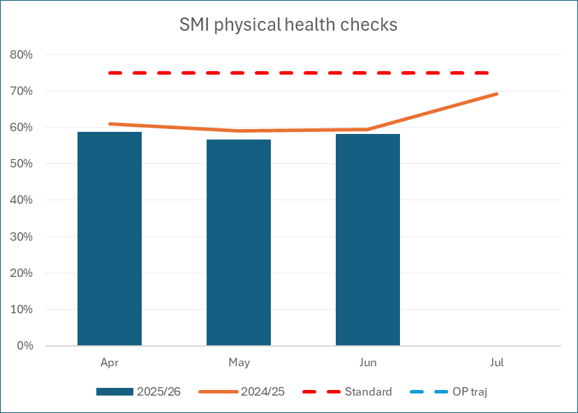
1.5.4.4. Severe mental illness (SMI)
This indicator monitors the proportion of people on the severe mental illness (SMI) GP register receiving six physical health checks within the last 12 months. People with SMI often have a lower life expectancy than the rest of the population due to preventable physical health problems. Therefore, a scheduled annual health check provides an additional opportunity for people with a diagnosis of SMI receive personalised support from their GP.
The Quarter 3, 2025/26 position showed that 58% of SMI patients in South West London received all six annual health check elements. NHS England required a minimum of 60% by March 2026 whilst working toward the national ambition of 75%.
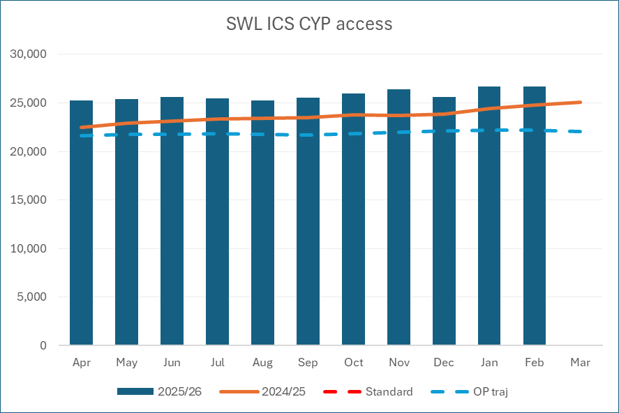
1.5.4.5. Children and Young People accessing Mental Health services
This indicator reports the number of children and young people, up to the age of 17, that have accessed appropriate services at least once in the last twelve months. Local NHS organisations were required to set a plan increasing the number of contacts for this group, supporting the national ambition of improving access to a range of services including mental health crisis, eating disorders, learning diability and autism.
South West London has exceeded its plan during 2025/26 with the most recent data showing 26,655 patients accessing services against a plan of 22,179.
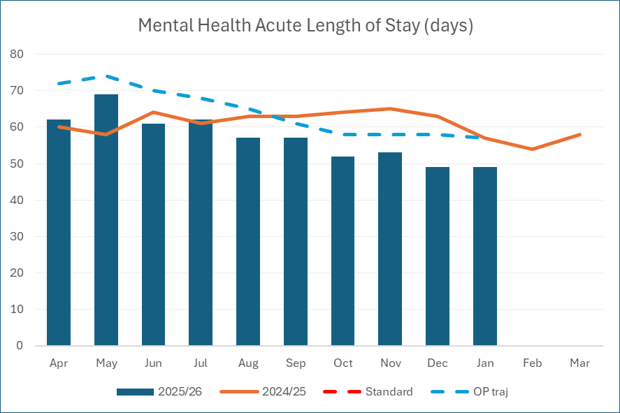
1.5.4.6. Average length of stay for patients in older adult mental health beds
This metric was introduced in 2025/26 to support the reduction in length of stay by improving discharge management and prevention of admission through increased utilisation of community mental health services. SWL ICB is on track in delivering its plan for the year. Improvement has largely been achieved by South West London and St George’s Mental Health NHS Trust (SWLSTG). SWLSTG have implenented a number of improvement actions, including a length of stay (LoS) framework which improves monitoring of patients progress at key milestones to bring forward discharge planning, access to rehabilitation services with clinical oversight.
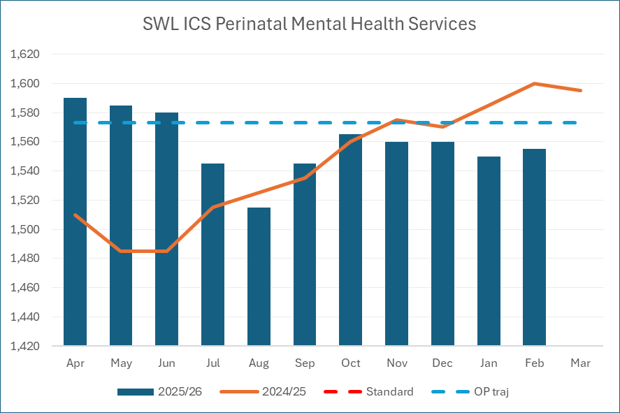
1.5.4.7. Access to perinatal mental health services
NHS Access to specialist perinatal mental health services, including Maternal Mental Health Services, provide life-saving care to women and birthing people impacted by severe or complex mental health problems during and after pregnancy. These services aim to ensure that women and birthing people receive the care and support they need to manage their mental health effectively, promoting their recovery and well-being.
The number of patients Accessing South West London ICB perinatal mental health services (rolling 12-month metric), increased annually to 1,555 patients (as at February 2026), which is slightly below plan by 18 patients.
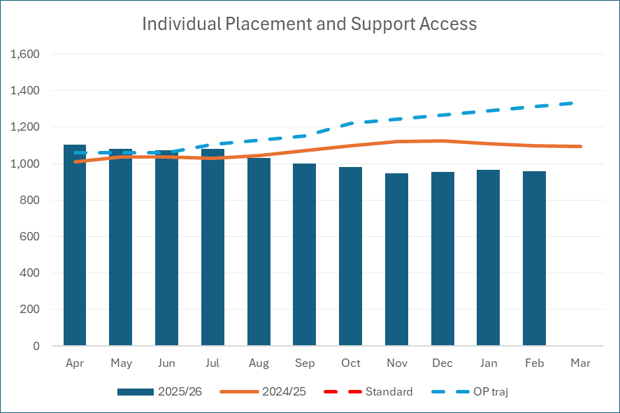
1.5.4.8. Individual Placement and Support (IPS) services
NHS IPS mental health services are designed to support individuals with severe mental health difficulties in finding and maintaining employment. These services are part of the NHS Long Term Plan and are integrated within community mental health services. IPS services are open to all who want to work, regardless of diagnosis or health conditions, and focus on finding meaningful and sustainable employment.
South West London ICB have achieved 72% of our 2025/26 plan, as of February 2026. Performance levels are lower as there have been fewer referrals to access IPS services compared to the previous financial year.
1.6. Overview of our key performance issues and risk
During 2025/26 the South West London Integrated Care Board refreshed its Board Assurance Framework (BAF) to strengthen alignment with the organisation’s strategic objectives and evolving role as a strategic commissioner. The updated framework focuses on the principal strategic risks to delivery of the ICB’s strategic objectives and provides clearer differentiation between strategic risks and those managed through the Corporate Risk Register, which relate to operational risks. The refreshed BAF also provides clearer visibility of controls, sources of assurance and areas where further development is required as the organisation continues to evolve.
The operating environment continues to present significant challenge. Financial pressures, increasing demand, workforce constraints and ongoing organisational transition continue to shape delivery of core objectives. Overall assurance across the BAF remains assessed as medium, reflecting that governance arrangements and controls are established, but many risks remain influenced by wider system dependencies and factors beyond the direct control of the ICB. Strengthened strategic risk oversight arrangements continue to support the Board in understanding these risks and monitoring progress.
A summary of the ICB’s principal strategic risks is provided below.
1.6.1. Statutory responsibility to oversee and secure a financially sustainable health and care system
Financial sustainability continues to represent a significant strategic risk for the system. South West London remains financially challenged and there is an ongoing risk that delivery of financial balance and a credible medium-term plan may not be achieved. System-wide financial recovery planning, strengthened budget-setting processes and oversight through the Finance & Planning Committee provide ongoing assurance, supported by regional scrutiny and regular Board review. Transformation programmes and productivity improvements remain central to delivery, with progress dependent on sustained system collaboration and alignment of planning assumptions. Assurance remains assessed as medium, recognising both the strength of governance arrangements and the scale of the financial challenge.
1.6.2. Urgent and emergency care
Urgent and emergency care remains an area of sustained operational pressure, with risk arising from increasing demand, workforce challenges and constraints across discharge and patient flow. Governance through the Urgent and Emergency Care Board, alongside targeted improvement programmes focused on access, flow and workforce, continues to provide oversight. Performance is monitored through integrated reporting across quality, finance and operational domains, enabling a system-wide view of pressures and emerging risks. Despite continued improvement activity, pressures across the pathway remain significant and assurance remains assessed as medium.
1.6.3. Oversight of contractual delivery (access, outcomes and constitutional standards)
Delivery of access to care and achievement of NHS Constitution standards continues to present risk across parts of the system. While progress has been made in elective recovery and performance monitoring, challenges remain in primary care access and mental health pathways. Governance arrangements supporting advice and guidance, patient-initiated follow-up and prioritisation of patients waiting longest remain in place to support recovery, alongside strengthened oversight of contractual delivery and performance expectations. Assurance for this risk remains medium.
1.6.4. System quality oversight
System quality oversight remains a priority as the ICB continues to evolve its operating model and navigate wider system pressures. The risk reflects the potential for deterioration in quality, safety and patient experience during organisational transition and ongoing operational demand. Strengthened quality governance arrangements, oversight forums and continued engagement with providers support early identification and escalation of risk. Continued alignment with system partners and evolving assurance arrangements aim to maintain robust oversight during this period of change. Assurance remains medium as arrangements continue to mature.
1.6.5. Interruption to clinical and operational systems as a result of a cyber attack
The risk of disruption to clinical and operational systems due to cyber threats remains a key consideration across the system. Increasing digital dependency, alongside variation in cyber maturity across partners, continues to shape this risk. Implementation of an ICS cyber strategy coordinated governance through the Digital Board and strengthened system-wide cyber assurance arrangements provide ongoing mitigation. Assurance remains assessed as medium as cyber resilience continues to develop across organisations.
1.6.6. Infrastructure capability across SWL
Infrastructure and estates capability continues to present a strategic risk, reflecting the need to align estate planning and capital investment with evolving clinical models and neighbourhood delivery. Delivery of a ten-year infrastructure strategy strengthened capital prioritisation governance and ongoing engagement with partners support long-term planning and system transformation. Assurance remains assessed as medium, with further work underway to optimise estate utilisation and support sustainable service delivery.
1.7. Improving quality and safety
We want high-quality, personalised, and equitable care for all, now and into the future.
1.7.1 Our ambition
We want to create a culture and environment that supports the delivery of high quality, continually improving care in which excellence in clinical care can flourish. We also believe that improving patient experience is as important as improving clinical outcomes and safety, especially we move towards our new role of strategic commissioning
Last year, our actions to achieve this included:
1.7.1.1. Safe care and system wide learning
We continued to strengthen implementation of the initiatives in the NHS patient safety strategy to support safety improvement including by:
- learning from patient safety event (LFPSE) national system
- Level 1 and Level 2 patient safety training as part of staff mandatory training
- supporting patient safety partners across all South West London organisations who are mandated
- embedding Patient Safety Incidents Response Framework (PSIRF) for providers who have transitioned and supporting piloting in general practice
- supporting local discussions on inequalities and harm
We have taken steps to strengthen continuous improvement and learning across the system through our system continuous improvement collaborative network (CIC) and have undertaken system show and tell visits events for each provider. The CIC network and show and tell visit events have focussed on sharing learning from quality improvement (QI) work implemented, strengthening leadership, building capacity and capability, implementing the Quality Management System (QMS) model and NHS impact
Through our system peer learning reviews, we have continued work with provider trusts to create safer systems of care that reflect continuous learning and improvement, understanding and learning from errors and excellence and adopting best practices.
We have revised and strengthened how we assess quality and equality impact across the system when we introduce changes through equality and quality impact assessment (EQIA).
In addition, we have continued to strengthen our ICB quality governance and have a system quality and safety group which brings together all partners across the system with a focus on sharing learning and improvement. We have seen key outputs from our system quality group (system quality council), system patient safety steering group and PSIRF community of practice, system patient safety partners network, system patient experience group, system medicines optimisation safety and learning network and system IPC committee.
1.7.1.2. Delivering effective care
We have continued to optimise use of the South West London quality dashboard, which ensures that National Institute of Clinical Excellence (NICE) clinical guidelines are reflected in how we measure outcomes.
As well, we have continued working closely with NICE to embed their guidance at system level, this is evolving work. Our work was recognized globally as a good exemplar of partnership working.
We have implemented a peer review framework to support system learning reviews, which is helping us develop safer systems of care that reflect continuous learning and improvement and reduce unwarranted variations in clinical care.
1.7.1.3. Experience and outcomes for patients and staff
Supporting our system partners to strengthen patient experience of care, use of feedback, compliments, and complaints to improve the quality of our health and care services. For example, we have a patient experience group with representation from all our patient experience leads. The group’s focus is using insights and data to improve patient experience, implement personalised and targeted initiatives and support system-wide learning and improvement.
In the last 2 years, we have seen all our patient safety partners (PSP):
- gain confidence in their new roles supporting patient safety activities in their organisations
- being involved in safety incidents reviews
- championing the PSP role to staff
- taking part in safety audits and reviews
- support patient safety groups and committees.
1.7.2 Our quality statutory duties
1.7.2.1. Safeguarding
ICBs have several key safeguarding responsibilities to ensure the safety and welfare of children, young people, and adults at risk.
We have executive and designated roles to represent the health community in both Safeguarding Adult Boards and Safeguarding Children’s Partnerships and sub-committees, working with Police, Local Authority and education colleagues, along with our partner organisations in health to support in the delivery of our safeguarding requirements and drive improvement.
In addition, we ensure delivery of the NHS Safeguarding Accountability and Assurance Framework (SAAF), which outlines the roles and responsibilities of NHS staff in safeguarding children, young people, and adults at risk, and sets out key priorities to keep people safe from abuse.
To meet our safeguarding duties this year, our work has included:
- Working with providers to ensure that all South West London commissioned organisations meet their statutory safeguarding responsibilities, with clear leadership and lines of accountability, appropriate policies and procedures, and safeguarding training so that children and adults at risk of harm are protected.
- Ensuring that the voice of the child, family and adult is central to all areas of work, learning and development and taking innovative approaches
- Supporting the delivery of actions resulting from safeguarding practice reviews, Domestic Homicide Review and other cases for learning, ensuring improvements take place across the system.
- Ensuring that the assurance frameworks which were developed last year are embedded into all contracts and strengthened the safeguarding role within the procurement process to drive up standards in safeguarding across all providers.
- Working with our community safety partnerships and provider organisations to support the reduction of serious violence within the healthcare setting and beyond. We have published our shared improvement plans which include the health responsibilities.
- Improving the potential to identify victims of domestic abuse through enhanced training in primary care for both clinical and non-clinical staff and via closer working with independent domestic violence advisors working with primary care teams
- Rolling out the standardised safeguarding protocols for pressure ulcers, falls and medication related errors to support standardising the approach across South West London and help the decision making of front-line staff.
- Establishing a mental capacity and deprivation of liberty forum to support improvements to practice, strengthen community arrangements and support children’s services in compliance.
- Supporting primary care with our named GPs ensuring strong, multi-agency working and case-based learning to support improvements in practice.
About safeguarding adults in South West London:
- Croydon:
- Kingston:
- Merton
- Sutton:
- Richmond and Wandsworth:
About safeguarding children in South West London:
- Croydon:
- Kingston and Richmond:
- Merton:
- Sutton:
- Wandsworth:
1.7.2.2. Children Looked After
A child looked after is a child who has been in the care of their local authority for more than 24 hours. They can live with foster parents, in a children’s home, or in a residential setting.
Many of these children may have a range of both physical and mental health needs. The ICB has responsibility to ensure the health needs of these children are met and will work with providers of health and care to support this delivery.
To support children looked after we have:
- Continued to work as corporate parents with the Board and engage directly with children looked after and care leavers, ensuring their voice and experience is heard.
- Continued work with health providers and local authorities to look at the pathways for initial health assessments and reviews to ensure that assessments and reviews are undertaken in a timely manner as per national guidance. Pathway reviews and action plans were developed for a number of areas, and identifying best practice nationally will continue in 2025/26.
- Delivered our free prescription offer for care leavers and widened this to provide support for dental and ophthalmic provision across South West London.
- Recruited four care leavers into the ICB, and promoting the development of processes across the wider system to enable other organisations to progress our commitment to support care leavers into employment.
- Supported improvements in the health provision for children looked after across a range of services from mental health to physical health provision.
- Developed and implemented a standardised approach and framework for Review Health Assessments to drive up standards of care.
- Carried out a Health Needs Assessment of Children Looked After to inform strategic commissioning intentions and deliver the necessary improvements to achieve better health outcomes for all children looked after.
1.8. Research and innovation
Research and innovation are fundamental to advancing healthcare, as they enable the development of new treatments, approaches, and technologies that improve patient outcomes and enhance service delivery. The South West London Integrated Care Board facilitates and promotes research through the South West London Health Research Collaborative which works to deliver the South West London Research Delivery Plan.
The collaborative is chaired by the ICB and made up of research leads from the community, acute and mental health trusts, Health Innovation Network South London (HIN), South London Allied Research Collaboration (ARC), South London Regional Research Delivery Network (RRDN), Big South (South London Partnership), Health Watch, voluntary sector, local authorities and our five universities. The plan covers six workstreams:
- Workforce – grow, develop and support research capacity in the system, including education and training, prioritising people’s time to do research in trusts, ICB, primary care & local authorities and developing community research careers.
- Needs and Priorities – helping each other to identify the specific priorities to research through JSNAs, ICP strategy, JFP, Core20PLUS5, NHS Long Term Plan & Local Health and Wellbeing plans; identifying digital needs and using population health management and coproduction to amplify community voices.
- Participation & Involvement – helping everyone to use, be part of and do research. This includes increasing the public’s research literacy, public and community participation and diversity in participation in SWL; developing peer researcher careers (people with lived experience) and research involvement in communities.
- Evaluation – all ICS (NHS, LA & voluntary sector) staff are enabled to deliver robust and relevant evaluations with evaluation included in the planning of projects; project leads are facilitated to access evaluation support including rapid evaluation
- Implementation of research findings – working together to ensure SWL ICS staff (NHS, LA, voluntary sector) apply existing research findings/evidence that are effective into their policies, programmes and practices and set up a governance structure that works for knowledge sharing, transfer and mobilisation
- Knowledge and information – improve access to people who can do rapid reviews, access to health data, population health management, NHS Research Secure Data Environment Network, knowledge mobilisation etc; develop knowledge exchange across SWL (2-way exchange between researchers and research users)
Examples of the work that the ICB has led over 2025/26:
- In May 2025, we hosted our first SWL Research Summit. Over 300 people came together, from the NHS, local authorities, voluntary, community and social enterprises (VCSEs), and universities, to showcase and celebrate the amazing research already happening across our boroughs.
- We are also developing peer researchers (people with lived experience) and community researchers to be an active part in this network as their lived experience and understanding of a social or geographical community can help generate information about their peers.
- The public health consultants in the ICB have been co-leads in several research bids – and have collaborated on research papers. This includes the NHSE funded study on digital exclusion in community pharmacies.
- The ICB is a GMC registered training location for public health, accommodating speciality registrars in public health and GP trainees. This provides opportunities for public health research.
- We have 7 GP practices in 2025/26 who are actively recruiting into clinical studies, and 5 clinical studies currently being done by GP practices. Although our recruitment figures are low as compared to other London ICBs, recruitment into studies has improved in South West London in 2026.
- We ran two research cafés with general practice staff to grow research literacy and to familiarise them with the EMIS tool to recruit patients into commercial studies.
- We also applied for and were successful in receiving strategic planning money from SL RRDN to work with the HIN SL to grow research capacity using an evidence-informed approach.
- In March 2026, South London overall had 1221 open studies in the Trusts. Whilst this is lower than the London average, the number of studies has remained stable overall.
1.9. Digital and population health management
We are using digital technology to transform care and improve patient outcomes across South West London. This includes promoting the health and wellbeing of our population and increasing the number of people that can live independently at home, for as long as possible. Our work focuses on five priorities:
- Innovation
- Personal health and care records
- Digital infrastructure
- Shared care records
- Population health platform
Population Health is an approach aimed at improving the health of an entire population. It is a focus on improving physical and mental health outcomes, promoting wellbeing and reducing health inequalities across an entire population, including a specific focus on the wider determinants of health (such as housing, employment, education). Population Health Management is the combination of data, tools and techniques that are implemented to improve population health outcomes. It uses a combination of data to inform planning and delivery of proactive care to achieve maximum impact. This includes the use of segmentation, risk stratification and impact modelling to identify local ‘at risk’ cohorts
Digital technology is helping us to address long-term challenges, by offering innovative solutions for more joined up services. Our Integrated Care System provides your local NHS access to increasingly rich data, which can be used to target those communities with the greatest need.
Population health management is crucial for the delivery of neighbourhood heath and care and to reduce health inequalities and improve the health and wellbeing of everyone in South West London.
1.9.1. Our ambition
As digital technology is now a significant part of our everyday lives, we want to facilitate the analogue to digital switch, by using technology to change the way we deliver services, ensuringbetter clinical capability for record sharing and case management holding and patient accessibility of their care record.
This will also improve productivity and interoperability for our clinicians and staff for better patient outcomes. Recognising that not everyone can or wants to engage with the NHS digitally, we aim to offer a range of ways for people to access care and support.
This year, our actions to achieve this included:
1.9.1.1. Working to empower patients and people to take control of their own health and wellbeing in partnership with health and care professionals
- Promoted use of the NHS app (Primary Care) and now have more than 1 million people registered in South West London, which is 71% of our 13+ GP registered population.
- Use of the app has improved the availability of information for both patients and clinicians at the point of care by empowering them with tools to support themselves to self-care and make informed choices about their treatment with functionality to book GP and hospital appointments, order repeat prescriptions, get test results and view personal GP records.
- Self-care at home has also progressed through virtual care, such as innovative Virtual Wards with a dedicated nurse led remote monitoring hub, and the use of technology in patients’ homes.
1.9.1.2. Working collaboratively across organisational boundaries to seamlessly support individuals
- Continued to expand our patient engagement portal (Secondary care), which integrates with the NHS App with St George’s University Hospital Trust one of the first to go live. With over 500,000 patients registered across South West London, they can now check their appointments and average waiting times (Kingston and Richmond piloted before successful nationally). It also helps the NHS manage and validate waiting lists and support patient-initiated follow up (PIFU).
- Continued the implementation of our three-year digital transformation plan which included the Cerner Millennium electronic patient record being implemented at Epsom and St Helier University Hospitals NHS Trust to align their systems with St George’s University Hospitals NHS Foundation Trust in May 2025
- Collated a three year South West London Digital Transformation Investment Portfolio, with the creation of multiple working groups focusing on the collaboration and convergence of digital health and care and infrastructure improvements across the system, working towards joined-up digital platforms to enable staff seamless access to systems, patient information and clinical systems they need, wherever they are.
- Developing a South West London Artificial Intelligence (AI) capability, including an AI Oversight group, aimed at ensuring alignment with the Pan London AI Adoption Framework and governance with system partners around AI, Robotic Process Automation (RPA) initiatives. This year we have worked with our providers to procure Ambient Voice Technology which will begin implementation in Spring 2026.
- Continued work on the foundations of our data strategic plan, which describes how the NHS and local authority partners across South West London are working together to support delivery of joined up, person-centred care across our health and care system. Achievements this year include:
- Supporting the implementation of London’s Secure Data Environment and working closely with other London ICBs to migrate health data to the new platform
- Optimising analytics and the business intelligence team and developing our community of data specialists in south west London – to develop our data capability, maximise in-house expertise and support workforce development.
- Changing the culture of how we use data, ensuring that we have timely access to data and the appropriate tools to interrogate it.
- Improving access to good quality data (Delivery of data environments – optimising use of data at scale) and creating robust governance for data (foundations to deliver the seven priorities for data set out in our data strategic plan for all partners) underpinning how we work – to create a single version of truth for data across all system partners.
1.9.1.3. Working to develop a data driven system that tackles inequalities, improves population outcomes, and drives up productivity
- Over the past year, we have been working on embedding population health management as part of the new integrated neighbourhood teams. Under the guidance of Neighbourhood Health Guidelines 2025/26, NHS England’s Core20PLUS5 approach and the ICB Strategic Commissioning Framework, we are working with OneLondon to ensure ICB commissioning and neighbourhood developed is guided by population segmentation and risk stratification, to ensure commissioning models take a person-centric approach to address the drivers of risk and have a sharp focus on equity in access, experience and outcomes.
- We continued to apply a single, consistent system-wide population health management method to our ICB analytics platforms to segment and risk stratify populations, based on complexity and forecasted resource use. This approach continues to be supported by a system-wide intelligence function.
- Our PHM methods on the ICB analytics platforms were reviewed in 2025/26 and found to have high level outputs. There is rapid identification of the main drivers of resource utilisation within the population, supporting further prioritisation of targeted interventions. Work is ongoing to build a more comprehensive model, introducing proxy measures of need and utilising supervised and unsupervised machine learning to run predictive impact modelling. Working to secure transformation and learning
NHS South West London has an ambition in our Joint Forward Plan to be a learning health system and to create a safer system of care that reflects continuous learning and improvement. We can demonstrate this through:
- The Patient Safety Incident Response Framework, PSIRF, transition: In 2023, all of the NHS organisations in South West London transitioned to work under the Patient Safety Incident Repose Framework, PSIRF. PSIRF is a learning model that supports developing and maintaining effective systems and processes for responding to, learning from and improving patient safety incidents.
- We have commenced trust and providers site visits across South West London using a learning framework that allows providers to share what works well and where there may be areas of improvement. This framework has been successful in evaluating the safety of our services and we have rolled the framework out to our continuous improvement clinical and non-clinical leads across South West London to ‘show and tell’ the system of their improvement journey.
- We have strengthened our system learning networks and through some of these core communities of practice, learning continues to be shared widely to improve patient safety and quality in South West London:
- System Patient Safety Steering Group and its Community of Practice
- Medicines Optimisation Safety Learning Group (MOSLIN)
- Continuous improvement Collaborative
- System Patient Safety Partners Network
1.10. People
1.10.1. Workforce
We want health and care services in South West London to be a great place to work for all our staff. We need to work in a more integrated way, making sure that our people are supported to have more flexible careers, a better work-life balance, and that we have the right numbers of people with the right skills to meet the changing needs of our populations
National reform has reshaped the role of Integrated Care Boards and required reductions in running costs. In South West London, this has meant reviewing how we are organised and beginning a process of redesign in line with South East London. We recognise the uncertainty this has created, and remain grateful to colleagues for their professionalism and commitment throughout this period.
We are committed to supporting staff through the current changes and have introduced several initiatives in response to staff feedback to help navigate change, develop skills, and embed our shared values. This includes strengthened learning and development offers, guidance on career transition, and more accessible health and wellbeing support.
You can read more about how we are supporting colleagues through change in section 2.7 Staff report.
1.10.2. Belonging and inclusion
Our vision is to make South West London a great place to work and live, where everybody feels included and that they belong. In response to the current financial and operational context, we have intentionally reshaped our approach to Equality, Diversity and Inclusion (EDI). While the delivery model has changed, our commitment to creating an inclusive culture remains unchanged. The EDI Programme Director continues to provide advice and support to colleagues across the system.
We are prioritising statutory compliance, embedding equality within governance and organisational change processes, and focusing on sustainable activity that supports both our workforce and our communities.
1.10.2.1 Supporting Staff Through Organisational Change
As the system prepares for a period of organisational consultation, the EDI programme has supported early engagement activity through a series of listening events with staff. These sessions have created space for colleagues to share their perspectives and concerns, helping to inform the approach to the forthcoming consultation.
As the process progresses, equality, diversity and inclusion considerations will continue to be woven throughout the consultation and change process. This includes supporting leaders to consider the potential impact of proposals on different staff groups, advising on inclusive engagement approaches, and ensuring equality impact assessments and governance processes are appropriately applied. The EDI programme will also contribute to consultation panels where appropriate, providing constructive challenge to support fairness, transparency and consistency in decision making.
1.10.2.2. Supporting International Staff
The ‘Ask Aunty’ app continues to support international healthcare staff by providing access to pastoral, cultural, psychological and emotional wellbeing support.
1.10.2.3. Supporting Staff with Disabilities
The Disability Advice Line (DAL) supported staff with disabilities and long term health conditions by providing guidance and information to managers and staff, aligning with the NHS Workforce Disability Equality Standard and legal duties under the Equality Act 2010. The service concluded at the end of 2025 following a period of operation supporting colleagues across the system.
1.10.2.4. Celebrating Culture and Faith
We recognised key cultural and faith events including Black History Month, Chinese New Year, Pride, South Asian Heritage Month and Disability History Month through internal communications and engagement activity.
1.10.3. Our role as an anchor institution
The NHS is the largest employer in South West London, with many more employed in health and care roles in our council, voluntary and community sector and private health and care partner organisations across South West London. Our role as an anchor institution makes us best placed to help in strengthening the employment prospects and opportunities for underrepresented groups in our local communities.
The following programmes are supporting the ICB to deliver in our capacity as anchor institutions across South West London:
- Over the last three years, we have used our Mayor’s Skills Academy and Anchor Institution roles to widen participation in NHS careers, create accessible entry routes developed high-quality project-based work experience, and strengthened links between employers, education, and communities. This has established a strong, practical foundation for inclusive workforce growth.
- As part of our commitment to the Care Leavers Covenant and NHS Universal Family Programme, we recognised that traditional recruitment processes can disadvantage care-experienced people, so we introduced a simplified, values-based application approach. Through a pilot with Local Authority care leaving teams, we received 63 applications and appointed four care-experienced young people into safeguarding apprenticeship roles.
- We have focused on culturally informed engagement to better reach underrepresented groups for recruitment – including Black, Asian and minority ethnic communities, carers, care leavers, refugees, young and deaf and disabled people. This insight has shaped professional content and a targeted social media approach, using relevant channels and trusted influencers to encourage more people to consider careers in health and care.
- The South West London ICS apprenticeship programme has been running for over three years, helping managers better understand apprenticeships, increase levy utilisation and strengthen partnership working. More recently, the ICB has refreshed the apprenticeship strategy to improve apprenticeship pathways and education provision across the system.
- We have worked with the Department for Work and Pensions, further education colleges and the voluntary sector to support local people through NHS careers awareness and application sessions, and engaged 3,500 people at South West London careers events focused on underrepresented groups.
We have continued to develop our partnerships across health and care, the voluntary sector and other Anchor partners, such as our universities. We have incorporated social value in procurement and supported a wide range of voluntary and community sector groups who work with our diverse communities to support people experiencing health inequalities across the wider determinants of health.
At the South Listens Health Assembly held in October 2025, leaders from South West London ICB restated their commitment to improving the process for raising health-related housing needs, and the creation of affordable housing on NHS land.
1.11. Complaints
Between 1 April 2025 and 31 March 2026, we received 845 formal complaints. Of these:
- 226 related to issues for which NHS South West London was responsible for investigating and responding to
- 352 were in relation to primary care, including GPs, dentists, pharmacists and opticians. Complaints relating to primary care became the responsibility of NHS South West London from 1 July 2023, having previously been managed by NHS England.
- We also received 267 complaints relating to issues which we are not directly responsible for, which were forwarded to the appropriate organisations for investigation and reply.
Of the complaints we received in this period, 4 have been referred to the Parliamentary and Health Service Ombudsman.
For those complaints that were within our remit, the most common complaints were about:
- Appointments, record keeping, Care & Treatment & referrals – 72
- Assessments & All age Continuing Care/CYP CC – 36
- Funding, Individual funding requests, IVF, medicines related concerns – 34
- Communications – 15
- Commissioning and waiting times – 30
- Staff Issues, aggression, values and behaviours – 4
- Service delivery concern and patient care – 13
- Complaints Handling – 8
- Medication and pharmacy – 1
- Adult Mental Health – 16
- Information Governance concerns – 3
We very much value the views of patients and other people who experience the services we commission. We consider any complaint or enquiry about these services as a vital part of reviewing and, where necessary, improving them. We are putting together a ‘learning from complaints’ framework that will allow us to improve the experiences of our patients.
1.11.1. Patient Advice and Liaison Services (PALS)
Members of the Patient Advice and Liaison Service (PALS) always listen carefully to the concerns raised by patients and their loved ones, and provide advice or make recommendations, where possible, as to the best way forward for the patient or member of the public.
While it is not always possible to resolve a concern to the service user’s satisfaction, the PALS team can give information about support services and voluntary organisations that may be able to help.
We believe that a successful PALS service helps reduce anxiety for those who use our services and helps people navigate the health and care system, whilst also reducing the number of issues that go on to become formal complaints.
The Complaints and PALS service also deal with a significant number of enquiries and informal concerns, from the public and MPs.
During this period there were 893 such contacts. The most common contacts related to:
- Redirections (inc. other NHS organisations) – 415 contacts
- Primary care (GPs, NHS dentists, community pharmacies) – 141 contacts
- General patient enquiries – 125 Contacts
- Funding, Individual funding requests, IVF, medicines related concerns – 30 contacts
- Continuing healthcare (assessment for eligibility process, payment) – 28 contacts
- General commissioning – 27 contacts
- Mental health commissioning (access to services and availability) – 26 contacts
- Vaccines – 23 contacts.
- Availability of medications (inc. NHS availability) – 10 contacts
Get in touch with PALS
We very much value your views, and use your feedback to help improve healthcare for everyone in South West London. You can contact PALS Monday to Friday between 9am and 5pm:
1.12. Environmental matters and sustainable development
The NHS started its decarbonisation journey in 2020 and is a significant contributor, nationally accounting for 4% of total UK carbon emissions. The NHS is working towards Net Zero by 2040 for emissions directly controlled and 2045 for those indirectly controlled.
The South West London NHS Green Plan (2025/26–2028/2029) sets out our short-term strategy (3-year horizon) for achieving net zero and mitigating against climate risks, building on momentum in prior years and adopting the concept of “Care Without Carbon”. The strategy is operationalised through eight workstreams and three cross-cutting themes, covering the areas of clinical transformation, digital innovation, travel and transport, estates and waste management, medicines optimisation, supply chain sustainability, workforce and leadership, and climate adaptation. These strategic priorities have targets, objectives and actions set for colleagues across the system to deliver, with clear ownership and responsibility. They are aligned to wider system strategies including the NHS Joint Forward Plan and the Integrated Care Partnership strategy.
Information provided in this section is in accordance with the DHSC GAM which sets out a phased approach to incorporating the recommended Taskforce on Climate-related Financial Disclosures (TCFD) as part of sustainability annual reporting requirements for NHS bodies, stemming from HM Treasury’s TCFD aligned disclosure guidance for public sector annual reports.
The ICB reports on the targets set in the system green plan. We are not required to disclose scope 1, 2 and 3 greenhouse gas emissions under TCFD requirements as these are computed nationally for local NHS bodies, by NHS England.
1.12.1. Achievements 2025/2026
Strong progress has been delivered against Year 1 of the 2025-29 SWL NHS Green Plan, with organisations collectively achieving 14 of 17 targets. Activities have set in motion an estimated 5,478 tCO2e per annum reduction and £2.3m in annual revenue savings, reflecting the continued commitment of partners across the system to the green agenda and progress against previously reported carbon emission reductions.
Some notable highlights include:
- Green Infrastructure Investment– c.£32m of additional capital funding was secured by SWL NHS organisations in 2025/26 to support estates decarbonisation and energy efficiency initiatives across the system.
- Expanding sustainability training – 647 people accessed sustainability training this year, significantly exceeding the target of 200 and reflecting the hard work that sustainability teams have put into developing and tailoring training and the enthusiasm that NHS staff have for this work.
- “Care without carbon”– Sustainability teams across the system delivered 37 projects to improve the sustainability of healthcare services, including sustainable theatre practices, “gloves off” campaigns and reductions in single-use items.
- Green Plans – All SWL trusts have now approved updated green plans aligned to the system-wide NHS green plan, strengthening our ability to track progress, share learning and coordinate delivery.
1.12.2. Governance
The SWL NHS Green Plan established governance structures and clear ownership that support collaboration with partner organisations. To support the journey towards net zero, performance is measured against a suite of climate-related metrics aligned to both national requirements and local priorities. A system-wide Green Plan Delivery Group meets monthly to progress these actions and targets.
The ICB Board and its committees receive six-monthly progress reports on the SWL NHS Green Plan, which set out performance and risks allowing for effective scrutiny and integration with wider organisational priorities.
Climate-related risks are integrated into the ICB’s risk management framework and are regularly reviewed. All trusts in our system have commenced work on climate risk through the completion of the NHSE Adaptation Risk Assessment Toolkit. Completing this and developing adaptation plans is a key priority in 2026/27.
Further details are set out in the SWL NHS Green Plan 2025-2029 and the six-monthly reports to the ICB Board.
1.12.3. Ambition for 2026-2027 and beyond
Across south west London, we are fortunate to benefit from passionate staff who are committed to this agenda with a great interest in innovations who have helped contribute to our achievements this year.
We will continue to work towards the NHS interim targets of an 80% reduction in direct emissions by 2028–2032 and showing progress towards an 80% reduction in indirect emissions by 2036–2039, and ultimately, full achievement of the NHS net zero target for direct emissions by 2040 and for emissions we indirectly control by 2045.
This will be achieved through greater scaling and full implementation of initiatives already commenced through, for example, wider adoption of heat decarbonisation and energy efficiency measures, greater prevalence of clinical models designed around net zero, the better leveraging of our supplier decarbonisation, better recognition and preparedness in adaptation planning and wider adoption of “Greener by Design” in commissioning, transformation and procurement decisions. SWL organisations will continue to plan towards these medium to long term ambitions, continuing to work in partnership with trusts, local authorities and public health.
1.13. Capital investment
We have a financial duty to ensure that the system’s allocated NHS capital budget is not overspent. We have worked in collaboration with SWL NHS partners to follow a risk-based approach to prioritise expenditure within the capital budget for NHS trusts to ensure value for money and that our services and environments are safe and fit-for-purpose for patients, staff and the public.
In 2025/26, £165.6 million was initially allocated to South West London for NHS trusts, including £19 million of capital receipts from previous asset sales to reinvest in the Tolworth Hospital site redevelopment. In the context of the national capital framework changes and removal of the system capital envelope from 2026/27, HMT approved the deferral of these capital receipts of £19 million and in-year capital receipts of £4.5 million to future years to support the committed expenditure for the Tolworth programme. Additionally, NHSE increased the system envelope by £22.2 million for specific projects. The revised budget for NHS trusts for the year therefore became £164.4 million.
The draft position reported by trusts at month 12 was £162.5 million, a £1.9 million underspend against the revised budget. Spend largely related to delivering strong progress on the £107m Tolworth redevelopment, the maintenance and other critical replacement investment in estates, IT and medical equipment and supporting the operational delivery within our trusts.
A £3.4 million budget was also allocated from NHS England specifically for investment in primary care for replacement IT and maintenance of GP practices. The reported position against this budget in month 12 was £3.4 million.
National NHS England programmes provided South West London with national funding, in addition to its annual allocations, to drive forward the national agenda and support local priorities. Through NHSE bidding processes and approval of business cases, £80.1 million of investment was made by trusts and £1.1 million in primary care including:
- Investing in energy efficiency schemes across trusts, including de-steaming the plant at Croydon University Hospital and at Kingston Hospital, the installation of LED lighting and solar panels to better manage energy consumption, and EV charging points to support the shift to electric vehicles.
- Commencing a SWL Primary Care Utilisation and Modernisation programme, which aims to support general practices to make better use of their existing estates footprint and increase the capacity they have for clinical work.
- Reducing the critical infrastructure risk across the system provider estate, with £36m of additional investment.
- Improving performance against constitutional standards through better equipment and digitisation, with £23m of additional investment.
In 2026/27, the ICB’s stewardship role over the system capital budget changes. The ICB will continue to support investment in the utilisation and modernisation of the existing NHS estate, replacement of ageing equipment, digitisation of the NHS and net zero targets, with the aim to support trusts and primary care to keep patients safe and ensure that day-to-day operations continue.
1.14. Estates and infrastructure
Our infrastructure underpins how people access safe, high quality services, and failure in buildings, digital systems or workforce environments risks disruption, poorer outcomes and higher costs. To address this, we developed the 10 Year South West London NHS Infrastructure Strategy, approved in July 2024, setting out our ambition for smarter, greener and more efficient infrastructure across estates, digital, workforce and sustainability.
The detailed review confirmed significant system wide challenges—including backlog maintenance, inefficient estate utilisation, fragmented digital infrastructure and cyber risk, primary care capacity pressures, decarbonisation needs and limited system capability. It also highlighted that required investment exceeds available capital, reinforcing the need for a more strategic and value driven approach.
The recruitment of a dedicated estates and infrastructure team since early 2025 has accelerated the pace of delivery against the strategy and strengthened system capability in 2025/26. Improved intelligence, new primary care lease and rent review systems, and validated void space assessments are now enabling more effective control and targeted action. This work has already identified around £7 million of historic overpayments, with £2.1 million recovered so far and a further £2 million forecast in 2026/27, alongside a void reduction programme expected to deliver £2 million in recurrent annual savings from 2026/27.
In addition, the ICB further developed its 4-year pipeline of future investment opportunities and is working towards securing funding to deliver affordable increased capacity across the system’s primary care sites. Of the primary care investments that are in-flight, the new primary care development in New Addington completed in November 2025 and others are making good progress towards completion in future years. A number of developments across the trust infrastructure have been delivered. An overview of capital investment made in 2025/26 is shared in Section 1.13.
Strong progress has also been made in relation to the 2025-29 SWL NHS Green Plan; an overview can be found in Section 1.12.
Digital infrastructure continues to mature; supported by over £1 million of external NHSE funds secured for cyber security and joint digital procurements delivering £1.2 million in savings across three years. The system has progressed consideration of a long-term system-wide approach to Electronic Patient Records in SWL in support of 10 Year Health Plan ambitions and multi-year programmes are underway to make improvements to networks, devices, cloud and service management.
As the ICB adapts to deliver its responsibilities as a strategic commissioner, Estates and Infrastructure will continue to support service delivery. Through a more capable estates function, stronger data, and coordinated system delivery, SWL is making clear progress, unlocking efficiencies and improving resilience—creating the foundations for long term transformation despite ongoing financial constraints.
1.15. Engaging people and communities
Working in partnership with people and communities is central to our approach in South West London. By listening to local feedback and involving communities in the design of our work, we strengthen accountability and create meaningful opportunities for people to influence and improve the services they use.
Understanding the needs of our diverse communities, particularly those experiencing health inequalities, alongside people’s experiences of care is vital to improving health services and preventing illness.
1.15.1. Our engagement strategy and legal duty
Our people and communities strategy ensures that the voices of residents, patients and carers are central to decision-making across the Integrated Care System (ICS). We aim to:
- reduce health inequalities by better understanding the needs of local communities
- involve people early when considering changes to services
- work with community leaders and voluntary organisations to strengthen our understanding of lived experience.
The NHS has a statutory duty to involve the public in decision-making under the Health and Care Act 2022. This includes involving patients and communities in planning services, developing proposals for service change and decisions about how services are delivered. We work closely with Health Overview and Scrutiny Committees across our borough councils to ensure engagement activity supports transparent decision-making.
1.15.2. Impact of engagement in 2025/26
Engagement with communities directly informed a number of programmes and service developments across South West London this year. Examples include:
- Engagement with people experiencing mental health crisis helped shape a South West London crisis café service specification, including involvement of people with lived experience in the procurement process.
- Outreach in New Addington Croydon, informed the development of a proposed Community Diagnostics Centre in an area experiencing significant health inequalities.
- Engagement with parents and carers in Sutton informed improvements to the neurodevelopment pathway and the development of clearer information for families.
- Community research in Merton and Wandsworth on oral health informed dental service planning and a targeted dentistry campaign.
- Engagement with communities experiencing health inequalities identified language barriers in primary care, leading to further work to improve access to services.
1.15.3. How we engage with communities
We use a range of approaches to involve people and communities in shaping health and care services.
1.15.3.1. Community-led approaches
Working with voluntary and community organisations enables us to reach people whose voices are not always heard. Our Healthy Communities grants programme supported 87 local organisations to host engagement activities in trusted community settings, reaching more than 6,000 residents across South West London.
These conversations focused on issues such as cardiovascular disease, mental wellbeing, respiratory health and healthy lifestyles. Insights gathered from this work are being used by Integrated Neighbourhood Teams and clinical programmes to shape prevention initiatives and improve access to services.
Through our Digital and Health Fund, we worked with 26 voluntary organisations to explore digital barriers to healthcare. Conversations with nearly 1,000 residents are informing digital strategies across South West London, including the development of new technologies to support clinical services.
1.15.3.2. Listening events and community networks
We regularly bring together community organisations, voluntary sector partners and local leaders to discuss priorities and share insight from local engagement work.
In March 2026, more than 80 community organisations attended a South West London listening event where we shared updates on local programmes and tested emerging priorities for our strategic planning.
We also hosted a conference on developing an anti-racist approach to health and care, bringing together community organisations to share insight and help shape recommendations for the system.
1.15.3.3. Focus groups, interviews and community research
Targeted engagement helps us reach people from specific communities particularly those who have poorer experiences of services and those with poorer health and wellbeing outcomes.
For example:
- Engagement with carers in Richmond informed the development of a borough-wide Carers Charter based on feedback from more than 250 carers.
- Conversations with people experiencing homelessness in Merton highlighted barriers to accessing primary care, including language barriers and digital exclusion. The findings have informed local service planning and outreach initiatives.
- Engagement across South West London explored how language barriers affect access to primary care, helping to identify improvements needed in interpretation services and communication support.
1.15.3.4. Digital and online engagement
Digital engagement complements our face-to-face work by enabling more people to participate.
For example, an online survey and targeted interviews with service users helped inform the development of a new specification for crisis cafés across South West London. More than 270 people shared their views and helped shape the future model of support for people experiencing mental health crisis.
1.15.3.5. Communications and engagement campaigns
We also work with communities to raise awareness of health services and encourage people to access support when they need it.
This year we delivered targeted campaigns promoting dentistry, Pharmacy First and vaccinations. These campaigns combined community outreach, digital communications and paid advertising to reach people in areas experiencing the greatest health inequalities.
1.15.4. Infrastructure supporting engagement
We have governance arrangements in place to ensure that insight from communities informs decision-making.
Engagement activity is coordinated by the ICB’s communications and engagement team and overseen through our governance structures. Engagement plans and findings are regularly shared with the Integrated Care Board and partners across the system.
Our South West London People and Communities Engagement Group brings together colleagues from NHS organisations, local authorities, Healthwatch and voluntary sector partners to review engagement activity and share learning across the system.
We also work closely with borough-based Place committees to ensure local insight influences decisions about services and priorities.
1.15.5. Insight and learning
To ensure engagement insight is used effectively, we have developed a South West London Insight Bank. This online resource brings together engagement findings from across the system, helping health and care professionals understand what matters most to local communities and reducing duplication of engagement activity. More than 300 reports are now available through the insight bank, providing valuable evidence to inform commissioning and service design.
1.15.6. Working with Healthwatch and the voluntary sector
Partnership working with Healthwatch and voluntary organisations is essential to our approach.
Our six local Healthwatch organisations provide independent insight into people’s experiences of health and care services and help ensure community voices influence decision-making.
This year Healthwatch organisations carried out engagement with people who are d/Deaf or deafblind to understand whether changes to interpretation services in primary care had improved access. Their findings are helping inform improvements to communication support for patients.
The voluntary, community and social enterprise (VCSE) sector also plays a critical role in reaching communities and supporting community-led approaches to health and wellbeing. Across South West London there are more than 5,500 VCSE organisations providing support to local residents and helping to address health inequalities.
Working in partnership with Healthwatch and the voluntary sector enables us to reach more communities, gather richer insight and ensure services reflect the needs of the people they serve.
You can read more about in our Engaging with people and communities annual report on our website.
1.16. Addressing health inequalities
Moving towards health equity is a key priority nationally, regionally and locally. Reducing health inequalities is a central goal in the treatment-to-prevention shift set out in the NHS 10 Year Plan, fundamental to ICBs as outlined in the Model ICB guidance, and central across all stages of strategic commissioning. We have prioritised reducing health inequalities in both our South West London Integrated Care Partnership’s Strategic Plan and Joint Forward Plan.
Health inequalities refers to the differences in health outcomes between different population subgroups including differences in how long we live or healthy lifespan. Inequalities in health are largely due to inequalities in society and the unequal distribution of the social determinants of health. These occur across several demographics including gender, age, ethnicity, socio-economic groups, geography, religion and sexual preference. There are also inequalities in the use of healthcare relating to education, income and occupation.
Healthcare is also a determinant of health inequalities, so addressing differences in access to and use of services between population groups will help in reducing overall health inequalities. In South West London, we are doing this by working towards equitable distribution of our services and embedding prevention, community empowerment and self-care.
We have spent considerable time in improving our health intelligence on health and healthcare inequalities. During the 2024/25 annual assessment of ICBs, NHS England noted the development of the Health Inequalities Explorer Dashboard to identify potential areas of inequality. Throughout 2025/26, we have continued to improve this dashboard as well as other tools on our internal Health Insights platform. Throughout 2025/26, we continued to embed NHSE Core20PLUS approach for healthcare and worked through Place level Prevention and Health Inequalities Boards to execute local strategies for reducing health inequalities. You can read a full account of the work we have done to identify and prioritise health inequalities within our South West London population and our work during 2025/26 on our website.
2. Accountability Report

Andrew Bland
Chief Executive and ICB Accountable Officer
16 June 2026
2.1. Corporate Governance Report
2.1.1. Members report
South West London Integrated Care System (ICS), works to:
- Improve outcomes in population health and healthcare
- Tackle inequalities in outcomes, experience and access
- Enhance productivity and value for money
Help the NHS support broader social and economic development. The ICS works in partnership to deliver its four aims and is made up of The Integrated Care Partnership (ICP), The Integrated Care Board (ICB) and our six Places.
The Integrated Care Partnership (ICP), has been established by the Integrated Care Board and the six South West London Local Authorities as a statutory committee that brings together a broad alliance of organisations and representatives concerned with reducing health inequalities, improving the quality of services and care, health and wellbeing of the population.
This means that key partners responsible for managing health outcomes in South West London, i.e. provider trusts, local authorities, voluntary, community and social enterprise organisations, and other local partners across primary and secondary care, come together to make decisions about local health services by using their local knowledge to improve services and focus resources where there is greatest need.
The South West London Integrated Care Board is the statutory NHS organisation responsible for developing a plan for meeting the health needs of the population, managing the NHS budget and arranging for the provision of health services. The Integrated Care Board is overseen by a Board, which is the senior decision-making forum and is collectively accountable for the delivery of the Integrated Care Board’s responsibilities. Key decisions and functions reserved for the Integrated Care Board include agreeing the vision, values, strategic direction of the Integrated Care Board and determining actions that will improve health and health services for local people.
The Board includes members from key NHS providers, local authorities, as well as Non-Executive Members and Integrated Care Board Executives.
Sir Richard Douglas is the Chair of the Integrated Care Board.
Mike Bell was Chair of the Integrated Care Board until August 2025. Anne Rainsberry was Acting Chair of the Integrated Care Board from August 2025 until early February 2026.
As Chief Executive, Andrew Bland is the Accountable Officer for the Integrated Care Board.
Katie Fisher was Chief Executive until 31 January 2026. Non-Executive Members have specific areas of responsibility and chair committees of the Integrated Care Board.
2.1.1.1. Role of the ICB Board
The Integrated Care Board operates as a unitary board, which means that all Board Members are collectively and corporately accountable for organisational performance. The purpose of the Board is to govern effectively and in doing so, build patient, public and stakeholder confidence that their healthcare is in safe hands.
The Board is responsible for coordinating and supporting the provision of high-quality healthcare to the community, encompassing primary and secondary care services. It is the Board’s responsibility to ensure the organisation is successfully discharging its duties today and will continue to do so in the future. To do this the Board uses the information available to:
- plan effectively: look at what is driving changes in demand, identify services which can help tackle immediate and long-term conditions, reduce avoidable ill-health and eliminate inequalities – and in parallel ensure workforce and capital plans reflect these areas.
- manage resources: based on what the organisation knows about care needs across the system’s communities and strategic priorities, establish a focused set of delivery and outcome expectations to make the most effective use of budgets and resources.
- ensure high-quality care is being provided: understand the provider landscape across different services, the collaborative(s), place(s) and other dynamics between organisations and procure cost-effective services to improve outcomes and wider population health
- seek assurance about care being delivered: use timely, accurate information on the quality and efficiency of care provided to gain assurance on the services being commissioned, pre-empt any issues and identify areas of improvement.
- consider risks and mitigations: identify, evaluate and manage risks to the ICB’s strategic and operational objectives.
Our Board met in public three times between April 2025 and March 2026, either in person or virtually, and on each occasion we encouraged our community to attend in person or virtually as appropriate, to find out about the work we’re doing. Read about public board meetings and download the papers.
As part of the establishment of the Integrated Care Board, the Health and Care Act 2022 introduced a new duty for NHS organisations to have regard to the effects of their decisions on the ‘triple aim’ of better health and wellbeing (including its effects in relation to inequalities), improved quality of services (including the effects of inequalities in relation to the benefits that people can obtain from those services) and the sustainable use of resources. Our structures and governance ensure we meet the triple aim and are described throughout this annual report.
Effective working with people and communities is essential to deliver the triple aim. During the year, the principles of the triple aim have been embedded across the Integrated Care Board, including at Place (within boroughs) and through the Integrated Care Partnership as demonstrated in some of the following areas:
- Development of the Integrated Care Strategy and related priorities at system level.
- Engagement on the South West London Integrated Care Board’s Five-Year Joint Forward Plan.
- The South West London Health Inequalities Fund.
The ICB’s Board was established on 1 July 2022 by ‘The Integrated Care Boards (Establishment) Order 2022’. Under the NHS South West London Integrated Care Board Constitution and Standing Orders.
Read profiles of our board members
2.2. Our Board
2.2.1. Composition of the Board
Members of the Board are as follows:
| Members | Designation and organisation |
| Mike Bell | Chair, Non-Executive Member, SWL Integrated Care Board (until August 2025) |
| Dr Anne Rainsberry | Non-Executive Member, SWL Integrated Care Board. Acting Chair, SWL Integrated Care Board from August 2025 to early February 2026 |
| Richard Douglas | Chair, Non-Executive Member, SWL Integrated Care Board (from February 2026) |
| Katie Fisher | Chief Executive Officer, SWL Integrated Care Board (until end of January 2026) |
| Andrew Bland | Chief Executive Officer, SWL Integrated Care Board (from February 2026) |
| Jo Farrar | Partner Member, Community Services (Chief Executive, Kingston and Richmond NHS Foundation Trust) |
| Vanessa Ford | Partner Member, Mental Health Services (Chief Executive Officer, South West London & St. George’s Mental Health NHS Trust) |
| Cally Palmer | Partner Member, Specialised Services (Chief Executive Officer, The Royal Marsden NHS Foundation Trust) (until May 2025) |
| Jacqueline Totterdell | Partner Member, Acute Services (Group Chief Executive Officer St George’s, Epsom and St Helier University Hospitals and Health Group) (until May 2025) |
| Dr Nicola Jones | Partner Member, Primary Medical Services, Interim Medical Director |
| Andreas Kirsch | Partner Member, Local Authorities (Leader of Kingston- upon-Thames Council) |
| Dr Masood Ahmed | Non-Executive Member, SWL Integrated Care Board |
| Jamal Butt | Non-Executive Member, SWL Integrated Care Board |
| Martin Spencer | Non-Executive Member, SWL Integrated Care Board (until May 2025) |
| Robert Alexander | Non-Executive Member, SWL Integrated Care Board (from May 2025) |
| Helen Jameson | Chief Finance Officer, SWL Integrated Care Board (until December 2025) |
| Dinah McLannahan | Interim Chief Finance Officer, SWL Integrated Care Board (from December 2025) |
| Dr John Byrne | Executive Medical Director, SWL Integrated Care Board (until May 2025) |
| Elaine Clancy | Chief Nursing Officer, SWL Integrated Care Board |
| Matthew Kershaw | Place Member, Croydon (Chief Executive Officer and Place Based Leader for Health Croydon Healthcare Services NHS Trust) (until May 2025) |
| Dr Annette Pautz | Place Member, Kingston (Kingston GP) (until May 2025) |
| Shannon Katiyo | Place Member, Merton (Director of Public Health, London Borough of Merton) (until May 2025) |
| Jeremy DeSouza | Place Member, Richmond (Executive Director of Adult Social Care and Public Health (until May 2025) |
| James Blythe | Place Member, Sutton (Managing Director Epsom & St Helier NHS Trust) (until May 2025) |
| Mark Creelman | Place Member, Wandsworth (Executive Locality Lead, Merton, and Wandsworth) (until May 2025) |
| Karen Broughton | Deputy CEO / Director of People & Transformation, SWL Integrated Care Board (until May 2025) |
| Jonathan Bates | Chief Operating Officer, SWL Integrated Care Board |
| Charlotte Gawne | Participant, Executive Director of Stakeholder and Partnership Engagement and Communications, SWL Integrated Care Board (until May 2025) |
| Hannah Doody | Participant, Local Authorities (Chief Executive Local Borough of Merton) (until May 2025) |
2.3. Committees, including the Audit Committee
The Integrated Care Board has established four committees which are accountable to the Board. The delegated powers and responsibilities of the committees are as set out in the Scheme of Reservation and Delegation (SoRD).
The committees supported our Board to carry out its statutory duties. The SoRD sets out:
- Decisions and functions that are reserved to the Board as a whole.
- Decisions delegated by the Board to the Integrated Care Board committees.
- Decisions delegated to individual members and employees.
The Integrated Care Board remained accountable for all of its functions including those that it had delegated.
In discharging their delegated responsibilities, the Board and its committees were required to:
- Comply with the principles of good governance.
- Operate in accordance with the Integrated Care Board’s SoRD.
- Comply with the Integrated Care Board’s Standing Orders.
- Comply with the Integrated Care Board’s arrangements for discharging its statutory duties.
Where appropriate, the board has ensured that members have had the opportunity to contribute to the Integrated Care Board’s decision-making process through the membership group.
When discharging their delegated functions, the Board and committees operated in accordance with their approved terms of reference.
2.3.1. Audit and Risk Committee
The Audit and Risk Committee was responsible for providing oversight and assurance to the Integrated Care Board on the effectiveness of governance, risk management and internal control processes across the whole of the Integrated Care Board’s activities that supported the achievement of the Integrated Care Board’s objectives. A key purpose of the committee was to monitor the integrity of the financial statements of the Integrated Care Board and assure itself that relevant risks, particularly financial, are appropriately identified and managed within a robust system of internal control. The Committee was also responsible for seeking appropriate assurance on functions relating to arrangements for counter-fraud and audit work programmes.
2.3.2. Remuneration Committee
The Remuneration Committee’s main purpose is to exercise the functions of the Integrated Care Board relating to paragraphs 17 to 19 of Schedule 1B to the NHS Act 2006.
The Committee was responsible for advising the Board on the implementation of the Integrated Care Board Pay Policy including adoption of any pay frameworks, and in meeting their responsibilities to ensure appropriate remuneration for all employees including very senior managers/directors (including Board Members) and Non-Executive Members, excluding the Chair.
The Committee provides oversight of the nominations and appointments to Integrated Board member roles.
2.3.3. Finance and Planning Committee
The Finance and Planning Committee was responsible for ensuring that there is both a robust financial strategy and planning framework in place and to oversee the system planning and broader financial management, including the review of financial plans and the current and forecast financial position of the Integrated Care Board and Place budgets.
The Committee also aimed to understand the drivers behind any variances against the plans, ensure any risks have been identified, and mitigating actions had been taken to address these whilst providing assurance to the Board about delivery and sustained performance. A Financial Recovery Group was established to demonstrate our work and show accountability. Regular reports from the group were fed into the Finance and Planning Committee.
2.3.4. Quality and Performance Oversight Committee
The Quality and Performance Oversight Committee was responsible for ensuring the Integrated Care Board secured continuous improvement in the quality of services, against each of the dimensions of quality set out in the Shared Commitment to Quality and enshrined in the Health and Care Bill 2021. This includes reducing inequalities in the quality of care.
The Committee provided assurance to the Integrated Care Board, that there was an effective system of scrutiny, quality governance and internal control underpinning the effective delivery of its strategic objectives, and provision of sustainable, high-quality care. The Committee reviewed and escalated key performance risks to the Board, ensuing that there was system oversight of Performance including at Place and Collaborative level.
With the engagement of respective Committee Chairs, members and attendees, the Terms of Reference for the Audit and Risk Committee, Quality and Oversight Committee, Finance and Planning Committee and Remunerations Committee have been reviewed and updated where appropriate to ensure they are fit for purpose and meet the needs of the Integrated Care Board.
2.3.5. Membership and attendance at the Board and committees
Membership and attendance at the Board and respective committees is shown in the table below. All meetings were quorate or where this was not the case decisions were made in line with the Standing Orders.
Board members
| Name | Role | Meetings attended |
| Mike Bell | Chair, Non-Executive Member, SWL Integrated Care Board | 1/1 |
| Dr Anne Rainsberry | Acting Chair, Non-Executive Member, SWL Integrated Care Board | 3/3 |
| Richard Douglas | Chair, Non-Executive Member, SWL Integrated Care Board | 0/0 |
| Jo Farrar | Partner Member, Community Services | 3/3 |
| Vanessa Ford | Partner Member, Mental Health Services | 1/3 |
| Cally Palmer | Partner Member, Specialised Services | 1/1 |
| Jacqueline Totterdell | Partner Member, Acute Services | 1/1 |
| Dr Nicola Jones | Partner Member, Primary Medical Services | 3/3 |
| Andreas Kirsch | Partner Member, Local Authorities | 2/3 |
| Robert Alexander | Non-Executive Member, SWL Integrated Care Board | 2/2 |
| Dr Masood Ahmed | Non-Executive Member, SWL Integrated Care Board | 3/3 |
| Jamal Butt | Non-Executive Member, SWL Integrated Care Board | 2/3 |
| Katie Fisher | Chief Executive Officer, SWL Integrated Care Board | 3/3 |
| Andrew Bland | Chief Executive Officer, SWL Integrated Care Board | 0/0 |
| Helen Jameson | Chief Finance Officer, SWL Integrated Care Board | 2/2 |
| Dinah McLannahan | Chief Finance Officer, SWL Integrated Care Board | 1/1 |
| Elaine Clancy | Chief Nursing Officer, SWL Integrated Care Board | 2/3 |
| Dr John Byrne | Executive Medical Director, SWL Integrated Care Board | 1/1 |
| Karen Broughton | Deputy CEO/Director of People & Transformation, SWL Integrated Care Board | 1/1 |
| Matthew Kershaw | Place Member, Croydon, Chief Executive Officer, Croydon Healthcare Services | 0/1 |
| Dr Annette Pautz | Place Member, Kingston | 1/1 |
| Shannon Katiyo | Place Member, Merton | 1/1 |
| Jeremy DeSouza | Place Member, Richmond | 1/1 |
| James Blythe | Place Member, Sutton | 1/1 |
| Mark Creelman | Place Member, Wandsworth | 1/1 |
Audit and Risk Committee
| Name | Role | Meetings attended |
| Robert Alexander | Committee Chair Non-Executive Member, SWL Integrated Care Board | 4/4 |
| Jamal Butt | Non-Executive Member, SWL Integrated Care Board | 1 /4 |
| Dr Masood Ahmed | Non-Executive Member, SWl Integrated Care Board | 3/4 |
Finance and Planning Committee
| Name | Role | Meetings attended |
| Jamal Butt | Committee Chair Non-Executive Member, SWL Integrated Care Board | 7/7 |
| Robert Alexander | Non-Executive Member, SWL Integrated Care Board | 5/7 |
| Martin Spencer | Non-Executive Member, SWL Integrated Care Board | 1/1 |
| Helen Jameson | Chief Finance Officer, SWL Integrated Care Board | 6/6 |
| Dinah McLannahan | Chief Finance Officer, SWL Integrated Care Board | 3/3 |
| Jonathan Bates | Chief Operating Officer, SWL Integrated Care Board | 7/7 |
| Elaine Clancy | Chief Nurse, SWL Integrated Care Board | 3/3 |
| Fergus Keegan | Acting Chief Nurse, SWL Integrated Care Board | 4/7 |
| Mark Creelman | Place Executive, Merton and Wandsworth | 4/7 |
| Dr John Byrne | Executive Medical Director, SWL Integrated Care Board. | 1/1 |
Quality and Oversight Committee
| Name | Role | Meetings attended |
| Dr Masood Ahmed | Committee Chair Non-Executive Member, SWL Integrated Care Board | 6/6 |
| Jonathan Bates | Chief Operating Officer, SWL Integrated Care Board | 5/6 |
| Dr John Byrne | Executive Medical Director, SWL Integrated Care Board | 1/1 |
| Dr Nicola Jones | Interim Executive Medical Director, SWL Integrated Care Board | 5/6 |
| Elaine Clancy | Chief Nursing Officer, SWL Integrated Care Board | 3/3 |
| Fergus Keegan | Acting Chief Nursing Officer , SWL Integrated Care Board | 2/3 |
| Marion Endicott | Quality & Patient Safety Representative | 6/6 |
Remuneration and Nominations Committee
| Name | Role | Meetings attended |
| Dr Anne Rainsberry | Committee Chair (meeting 23.5.25) Non-Executive Member, SWL Integrated Care Board | 1/1 |
| Jamal Butt | Committee Chair (meeting 26.11.25) Non-Executive Member, SWL Integrated Care Board | 1/1 |
| Dr Masood Ahmed | Non-Executive Member, SWL Integrated Care Board | 2/2 |
| Mike Bell | Chair, SWL Integrated Care Board | 1/1 |
| Dr Anne Rainsberry | Non-Executive Member, SWL Integrated Care Board | 1/1 |
2.3.6. Register of Interests
The ICB operated a robust policy for the management of Conflicts of Interest.
All attendees were required to declare their interests as a standing agenda item for every ICB Board, Committee or meeting before the item was discussed.
To protect the integrity of decision-making, arrangements for managing conflicts of interest and potential conflicts of interest were established. These includes recusing potentially conflicted members from deliberations where appropriate, and / or ensuring material (papers) were not circulated to potentially conflicted members.
The ICB register of interests can be seen here: Declarations
2.3.7. Personal data related incidents
During the period, the ICB identified no Serious Untoward Incidents relating to data security breaches, that were reportable to the Information Commissioner.
2.3.8. Modern Slavery Act
NHS South West London Integrated Care Board fully supports the Government’s objectives to eradicate modern slavery and human trafficking.
Read our Slavery and Human Trafficking Statement
2.3.9. Statement of Accountable Officer’s Responsibilities
Under the National Health Service Act 2006 (as amended), NHS England has directed each Integrated Care Board to prepare for each financial year a statement of accounts in the form and on the basis set out in the Accounts Direction. The accounts are prepared on an accruals basis and must give a true and fair view of the state of affairs of the South West London ICB and of its income and expenditure, Statement of Financial Position and cash flows for the financial year.
In preparing the accounts, the Accountable Officer is required to comply with the requirements of the Government Financial Reporting Manual and in particular to:
- Observe the Accounts Direction issued by NHS England, including the relevant accounting and disclosure requirements, and apply suitable accounting policies on a consistent basis;
- Make judgements and estimates on a reasonable basis;
- State whether applicable accounting standards as set out in the Government Financial Reporting Manual have been followed, and disclose and explain any material departures in the accounts; and,
- Prepare the accounts on a going concern basis; and
- Confirm that the Annual Report and Accounts as a whole is fair, balanced and understandable and take personal responsibility for the Annual Report and Accounts and the judgements required for determining that it is fair, balanced and understandable.
The National Health Service Act 2006 (as amended) states that each Integrated Care Board shall have an Accountable Officer and that Officer shall be appointed by NHS England.
NHS England has appointed Andrew Bland the Chief Executive Officer to be the Accountable Officer of South West London ICB. The responsibilities of an Accountable Officer, including responsibility for the propriety and regularity of the public finances for which the Accountable Officer is answerable, for keeping proper accounting records (which disclose with reasonable accuracy at any time the financial position of the Integrated Care Board and enable them to ensure that the accounts comply with the requirements of the Accounts Direction), and for safeguarding the South West London ICBs assets (and hence for taking reasonable steps for the prevention and detection of fraud and other irregularities), are set out in the Accountable Officer Appointment Letter, the National Health Service Act 2006 (as amended), and Managing Public Money published by the Treasury.
As the Accountable Officer, I have taken all the steps that I ought to have taken to make myself aware of any relevant audit information and to establish that South West London ICB’s auditors are aware of that information. So far as I am aware, there is no relevant audit information of which the auditors are unaware.

Andrew Bland
Chief Executive and ICB Accountable Officer
16 June 2026
2.4. Governance Statement
2.4.1. Introduction and context
South West London ICB is a body corporate established by NHS England on 1 July 2022 under the National Health Service Act 2006 (as amended).
The South West London ICB’ s statutory functions are set out under the National Health Service Act 2006 (as amended).
The ICB’s general function is arranging the provision of services for persons for the purposes of the health service in England. The ICB is, in particular, required to arrange for the provision of certain health services to such extent as it considers necessary to meet the reasonable requirements of its population.
Between 1 April 2025 and 31 March 2026 the Integrated Care Board was not subject to any directions from NHS England issued under Section 14Z61 of the of the National Health Service Act 2006 (as amended).
2.4.2. Scope of responsibility
As Accountable Officer, I have responsibility for maintaining a sound system of internal control that supports the achievement of the South West London ICB’s policies, aims and objectives, whilst safeguarding the public funds and assets for which I am personally responsible, in accordance with the responsibilities assigned to me in Managing Public Money. I also acknowledge my responsibilities as set out under the National Health Service Act 2006 (as amended) and in the South West London ICB’s Accountable Officer Appointment Letter.
I am responsible for ensuring that the South West London ICB is administered prudently and economically and that resources are applied efficiently and effectively, safeguarding financial propriety and regularity. I also have responsibility for reviewing the effectiveness of the system of internal control within the ICB as set out in this governance statement.
2.4.3. Governance arrangements and effectiveness
The main function of the Board is to ensure that the Integrated Care Board has made appropriate arrangements for ensuring that it exercises its functions effectively, efficiently and economically, and complies with such generally accepted principles of good governance as are relevant to it.
The Integrated Care Board’s constitution sets out how it shall fulfil its statutory duties and the primary governance rules for the Integrated Care Board. It includes information on Board membership and governance arrangements in line with relevant guidance issued by NHS England and complies with the Health and Care Act 2022. Following extensive engagement with local stakeholders, and approval by NHS England, the constitution came into effect following the establishment of the Integrated Care Board on 1 July 2022. Following guidance from NHS England, the Board agreed revisions to the constitution in November 2024 which incorporated several small amendments.
2.4.4. UK Corporate Governance Code
We are not required to comply with the UK Corporate Governance Code. However, we have reported on our Corporate Governance arrangements by drawing upon best practice available, including those aspects of the UK Corporate Governance Code and the Corporate Governance in Central Government Departments: Code of Good Practice 2011 (HM Treasury and Cabinet Office) that we consider to be relevant to the Integrated Care Board.
2.4.5. Discharge of statutory functions
The arrangements put in place by the Integrated Care Board and explained within the corporate governance framework were developed to ensure compliance with all relevant legislation.
The Integrated Care Board has reviewed all of the statutory duties and powers conferred on it by the National Health Service Act 2006 (as amended) and other associated legislation and regulations. As a result, I can confirm that the Integrated Care Board is clear about the legislative requirements associated with each of the statutory functions for which it is responsible, including any restrictions on delegation of those functions.
Responsibility for each duty and power has been clearly allocated to a lead Director. Directorates have confirmed that their structures provide the necessary capability and capacity to undertake all of the Integrated Care Board’s statutory duties.
2.4.6. Risk management arrangements and effectiveness
The Integrated Care Board has a robust internal control mechanism to allow it to prevent, manage and mitigate risks. The risk assessment section describes our approach to risk management and appetite for risk, explaining the key components of the internal control structure. Alongside the Integrated Care Board’s governance framework and refreshed Board Assurance Framework (BAF), these arrangements underpin the ICB’s ability to control risk through a combination of:
- Prevention – the Integrated Care Board’s structures, governance arrangements, policies, procedures, and training minimise the likelihood of risks materialising
- Deterrence – staff are made aware that failure to comply with key policies and procedures, such as the Standards of Business Conduct Policy or the Fraud, Bribery and Corruption Policy, will be taken seriously by the Integrated Care Board and could lead to disciplinary action, or dismissal
- Management of risk – once risks are identified, the arrangements for ongoing monitoring and reporting of progress through the Committee structure to the Integrated Care Board ensures appropriate action is taken to manage risks.
We are actively working on fostering a culture where the consideration of risk appetite is a key aspect of our risk management discussions. We aim to ensure that the concept of risk appetite is consistently considered by executives and risk owners, helping to inform decision making and strengthen the overall risk management framework.
Risk management remains a standing agenda item at relevant committee meetings at both place and corporate levels. These discussions, supported by the Head of Risk, place leads and executive directors, ensure that risk management remains embedded within strategic discussions and organisational decision making. The involvement of senior leadership in regular risk discussions supports a dynamic and responsive risk management process, enabling the organisation to respond effectively to emerging risks and changing priorities.
The Board discusses key issues, including risk management, through its formal governance arrangements. Two public Board meetings are held each year, where Board Assurance Framework (BAF) risks and other key matters are presented in an open forum to support transparency and accountability. Through these arrangements, reporting remains accessible and enables stakeholders and the public to understand how risks are identified, monitored and managed across the organisation.
2.4.7. Capacity to handle risk
The Senior Management Team is responsible for oversight of the risk management process, its members review both risk registers and the Board Assurance Framework (BAF) as part of their business cycle, and the management of all Integrated Care Board corporate risks are overseen by an executive director. It evaluates the status of risks, identifies new risks, and monitors effectiveness of the Integrated Care Board’s board assurance and risk management control systems
The responsibilities of Directors and Committees are set out in the Constitution and the accompanying Scheme of Delegation, as well as the governance reporting lines. Timely and accurate information to assess risk and ensure compliance with the Integrated Care Board’s statutory obligations, is supported by the annual plan of committee work. The Board has rigorous oversight of the performance of the Integrated Care Board, via formal Board meetings, seminars and through assurances received from committees and audits.
The overall responsibility for the management of risk lies with the Accountable Officer. The Board collectively ensures that robust systems of internal control and management are in place. These arrangements, and the enhancements that have been made to them, are described in the Risk Assessment section of this report.
Risk management capacity continues to be developed across the Integrated Care Board. The statutory and mandatory training programme includes numerous elements relevant to risk management, including information governance, health and safety, fire safety, safeguarding adults and children and counter fraud. Staff have been invited, and attended a Risk Awareness workshop, conducted by the Head of Risk.
Board and Committee reporting arrangements prompt authors to consider that key aspects of risk have been reviewed.
2.4.8. Risk assessment
The Senior Management Team is responsible for oversight of the risk management process. It evaluates the status of risks, identifies new risks, and monitors effectiveness of the Integrated Care Board’s board assurance and risk management control systems.
The Audit Committee provides scrutiny and independent assurance to the ICB Board on the effectiveness of the Integrated Care Board’s board assurance and risk management processes.
The Board reviews the content of the BAF twice a year as a means of assessing the current level.
All other sub committees of the Board review those risks specific to their area and are made aware of significant changes to the risk register at each meeting.
Operational management of the BAF is provided by the Integrated Care Board’s Corporate Affairs team. Regular meetings are held with manager leads to review progress and performance of each of the priority areas and associated risks. In addition, a Risk Leadership Group has been established to strengthen strategic risk oversight, bringing together Executive Directors and subject matter experts to review principal risks, support the ongoing development of the BAF and ensure alignment with the organisation’s evolving strategic commissioning model.
The BAF forms the basis for the Board to assess its position regarding achieving its corporate objectives. It uses principal risks to achieve those objectives as the foundation for assessment. It considers the current level of control alongside the level of assurance that can be placed against those controls.
Risks are assessed to determine whether they represent a principal threat to delivery of the organisation’s strategic objectives, with residual risk score forming one component of that assessment alongside strategic impact and Board-level relevance. In practice, this includes:
- Risks with a significant residual score, for example those that score 15 and above.
- Risks that are growing in significance or that pose a material threat to delivery of key objectives and therefore require Board oversight.
The Integrated Care Board views risk management as key to the successful delivery of its business and remains committed to ensuring staff are equipped to assess, manage, escalate and report risks. This ensures a comprehensive overview of all the risks affecting the organisation and facilitates decision making about those risks that need immediate treatment and those that the organisation can tolerate for a specified amount of time.
The Integrated Care Board uses an NHS standard risk scoring matrix (CASU 2002) to determine the scales of impact and likelihood of adverse events. The scale is scored from 1–25 (with 1 being the least severe and 25 being the most). Risks continue to be managed at director level with oversight by the committee relevant to the risk, alongside oversight from the Audit and Risk Committee. This allows:
- The appropriate level of investigation and causal analysis to be carried out.
- Identification of the level at which the risk will be managed, the assigning of priorities for remedial action and determination of whether the risk will be accepted.
Using the residual risk rating (i.e. after controls are taken into account), in the most recent iteration of the refreshed BAF there are six principal strategic risks
- BAF001 Failure of the ICB to discharge its statutory responsibility to oversee and secure a financially sustainable health and care system
- BAF002 Urgent & Emergency Care
- BAF003 Oversight of contractual delivery (access, outcomes and constitutional standards)
- BAF008 System quality oversight
- BAF004 Interruption to clinical and operational systems as a result of a cyber attack
- BAF009 Infrastructure Capability across SWL
2.4.9. Other sources of assurance
2.4.9.1. Internal Control Framework
A system of internal control is the set of processes and procedures in place in the South West London ICB, to ensure it delivers its policies, aims and objectives. It is designed to identify and prioritise the risks, to evaluate the likelihood of those risks being realised and the impact should they be realised, and to manage them efficiently, effectively and economically.
The system of internal control allows risk to be managed to a reasonable level rather than eliminating all risk; it can therefore only provide reasonable and not absolute assurance of effectiveness.
While the Health and Care Act 2022 places responsibility on ICBs to manage conflicts of interest and publish their own Conflicts of Interest policy, which should be included in ICB’s governance handbook, NHS England’s engagement with local stakeholders suggests nationally-commissioned basic training would be of value to avoid unnecessary duplication across systems. NHS England will provide updated national e-learning modules on managing conflicts of interest in the context of the new ICB arrangements and also explore developing additional guidance on conflicts of interest in consultation with ICB Chairs.
Our governance structures are used to ensure effective oversight of operational and strategic decisions and compliance with the NHS regulatory environment. Details of the Board responsibilities and those of its committees are outlined above and described in further detail within the Constitution.
Ensuring effective risk management, financial management and compliance with statutory duties is high on the list of our priorities. We have implemented policies, systems processes, and training to reduce exposure in these areas and to ensure that we are legally compliant. Each committee and group oversees risks and policies relating to their area of responsibility. Clinicians and management work in partnership through the commissioning cycle, adding value and delivering outcomes, to ensure the procurement of quality services that are tailored to local needs and deliver sustainable outcomes and value for money.
The Integrated Care Board has established an effective organisational structure with clear lines of authority and accountability which guards against inappropriate decision making and delegation of authorities enabling the Integrated Care Board to meet its statutory duties and follow best practice guidelines. Work to ensure that we promote and demonstrate the principles and values of good governance and the review of governance related risks takes place at Senior Management Team meetings and assurance is provided by the Audit and Risk Committee to the Board with insight from Internal Audit.
The Committee also ensures that, in non-financial and non-clinical areas that fall within the remit of its terms of reference, appropriate standards are set and compliance with them is monitored. We have considered the effectiveness of our governance framework and processes and raised no significant concerns on governance related matters this year.
The system of internal control is based on an ongoing process designed to identify and prioritise the risks to the achievement of the policies, aims and objectives of the Integrated Care Board, to evaluate the likelihood of those risks being realised and the impact should they be realised, and to manage them efficiently, effectively, and economically.
The system of internal control has been in place in the Integrated Care Board for the year ended 31 March 2026 and up to the date of approval of the annual report and accounts.
2.4.10. Data quality
The Board regularly receives reports that cover financial, governance, compliance, performance and quality matters for the Integrated Care Board.
The Integrated Care Board has a business intelligence and performance function which monitors how local providers are performing against key performance indicators. This information is reported to the Board on a regular basis.
The data contained in the reports is subject to significant scrutiny and review, both by management and by Integrated Care Board committees. The quality of information received to direct decision making is also assured through South West London Business Intelligence and Analytics function. The Board is confident that the information it is presented with has been through appropriate review and scrutiny, and that it continues to develop with organisational needs.
2.4.11. Information governance
The NHS Information Governance Framework sets the processes and procedures by which NHS organisations handle data and information on patients and employees, in particular personal identifiable and sensitive personal information. The NHS Information Governance Framework is supported by a Data Security and Protection Toolkit (DSPT) and the annual submission process provides assurances to the Integrated Care Board, other organisations and to individuals that personal information is dealt with legally, securely, efficiently and effectively.
The Integrated Care Board is due to submit its DSPT in June 2026. The ICB previously published its DSPT in June 25 to ‘Standards Met’.
We place high importance on ensuring there are robust information governance systems and processes in place to help protect both patient and corporate information. We have established an information governance management framework and have developed robust information governance processes and procedures in line with the Data Security and Protection Toolkit. We ensure all staff and interim contractors undertake mandatory annual information governance training to ensure staff are aware of their information governance roles and responsibilities in line with the implementation of our information governance framework.
There are processes in place for the reporting and investigation of information governance breaches or suspected breaches. We have a developed and implemented information risk assessment and management procedures which is regularly reviewed via our information governance steering group chaired by our Deputy SIRO.
2.4.12. Business Critical Models
In line with best practice recommendations of the 2013 MacPherson review into the quality assurance of analytical models, we confirm that an appropriate framework and environment is in place to provide quality assurance of business critical models. Gaps in best practice are assessed regularly and progress to improve constantly monitored.
2.4.13. Third party assurances
The Integrated Care Board relies on a number of third-party providers (such as NHS SBS and NHS BSA) to provide a range of transactional processing services ranging from finance to data processing. Our requirements for the assurance provided by these organisations are reviewed every year. Appropriate formal assurances are obtained to supplement routine customer/supplier performance oversight arrangements.
2.4.14. Control issues
NHS South West London Integrated Care Board received services from a number of external providers and at the end of the year received a service auditor report from each of these:
- NHS Business Services Authority (BSA) – Electronic Staff Record (ESR) -Type II ISAE 3000 Controls Report
- Transformation Directorate within NHS England (previously NHS Digital) – Extraction and Processing of General Practitioner Data Services in England -Type II ISAE 3000
- NHS Business Services Authority (BSA) – Prescription Payments Process -Type II ISAE 3402
- Capita Business Services Limited – Primary Care Support England – Type II ISAE 3402
- NHS England South, Central and West Commissioning Support Unit – Calculating Quality Reporting Service (CQRS) National – Type II ISAE 3402
- NHS North of England Commissioning Support Unit – Payroll Services – Type II ISAE 3402
- NHS Shared Business Services Limited (SBS) – Finance and Accounting Services – Type II ISAE 3402
Where exceptions have been raised in these, we consider the impact on the Integrated Care Board and if appropriate add local controls to mitigate the impact of any weaknesses identified. We have shared these Service Auditor Reports with Internal Audit who do not consider there are any issues sufficiently significant to alter their view of the controls as designed and operating at the Integrated Care Board.
2.4.15. Review of economy, efficiency and effectiveness of the use of resources
The Integrated Care Board, through its meetings, retains primary oversight of the appropriateness of arrangements in place within the organisation to exercise its functions in an effective, economic and efficient manner. The Accountable Officer for the Integrated Care Board retains overall executive responsibility for the use of our resources.
The organisation has a number of key processes and internal mechanisms that provide assurance that we are operating within our statutory authority:
Within our constitution there are clearly defined standards for conducting business, Standing Orders, Scheme of Reservation and Delegation along with Prime Financial Policies that ensure the effective management and protection of assets and public funds.
Key policies are in operation in respect of contract management and procurement that ensure effective operational and financial performance whilst ensuring we operate within regulatory frameworks and reduce the likelihood and impact of risk.
There is a clearly defined process for the consideration of business cases and saving opportunities to ensure transparency and value for money is upheld.
The Commercial Procurement Advisory Group evaluates the robustness of proposed business cases before these are then considered by the Senior Management Team, Finance and Planning Committee or ICB Board.
The Quality and Oversight Committee is accountable for overseeing a robust, organisation-wide system of quality and performance.
The Finance and Planning Committee ensures that the finances of the Integrated Care Board are scrutinised to ensure budgets are managed in an appropriate and timely manner. It will ensure that the Board is fully aware of any financial risks which may materialise throughout the year. It works alongside the Audit and Risk Committee to ensure financial probity in the organisation.
These committees have on behalf of the Integrated Care Board, an overview of all aspects of finances (including capital spend and cash management).
NHS England’s assessment recognised the ICB’s strong leadership across the system, including effective partnership working, robust governance arrangements and leadership of service transformation and digital innovation. The assessment also highlighted the ICB’s continued focus on quality improvement, patient safety, clinical leadership and engagement with local communities.
2.4.16. Commissioning of delegated services (primary care services and specialised services)
South West London ICB has signed delegation agreements with NHS England for the commissioning of delegated primary care services and specialised services and held full commissioning responsibilities for delegated services during the 2025/26 reporting period.
To the best of the ICB leadership’s knowledge, all delegated services were commissioned in accordance with 2025/26 delegation agreements and national service specifications.
The ICB leadership is able to provide the necessary evidence of compliance with the delegation agreements, any associated developmental requirements and national service specifications, and to show how effectively the delegated function is operating (either directly or via multi-ICB working arrangements) should NHS England or a third party (e.g. external auditors) ask for such evidence.
2.4.17. Delegation of ICB functions
To enable effective decision making, the Integrated Care Board operated under its Scheme of Reservation and Delegation (SoRD), as agreed by the Board, which sets out how and where decisions are taken. The SoRD specified which functions are reserved to the Board, and which functions have been delegated to an individual, committee or other group.
The Integrated Care Board has an effective Governance Framework which supports and enables the Board to comply with its statutory functions and duties. As noted in the Member Profiles, the Board is constituted from a broad range of organisations from within South West London, either as full members, participants or observers of the Board. The Board was appointed in line with NHS England guidance and ensures we have a broad range of experience and expertise helping us to deliver an effective decision-making process.
In South West London, we have six ICS Places: Croydon, Kingston, Merton, Richmond, Sutton, and Wandsworth which are co-terminus with the respective six Local Authorities. Our Places allow the Integrated Care Board to join up and co-ordinate the development and delivery of services according to the needs of their local populations.
Each Place discharges its duties in accordance with the Integrated Care Board’s SoRD, and as such a robust model of governance has been developed to ensure clear and transparent decision-making at Place level which support the overall delivery of the Integrated Care Board’s statutory responsibilities.
2.4.18. Counter fraud arrangements
Counter fraud arrangements are in place in the Integrated Care Board to ensure compliance with standards set by the NHS Counter Fraud Authority Standards for Commissioners: Fraud, Bribery and Corruption.
- An accredited Local Counter Fraud Specialist (LCFS) is contracted to undertake counter fraud work proportionate to identified risk.
- The Integrated Care Board’s Audit and Risk Committee receives progress reports throughout the year and an annual report against each of the standards for commissioners.
- There is executive support and direction for a proportionate proactive work plan to address identified risks.
- Regular fraud related communications are shared with Integrated Care Board staff and training is delivered to all staff.
- The LCFS meets with the Chief Finance Officer and Internal Audit to agree tasks to be undertaken as part of the workplan.
- The LCFS also has regular liaison with the Chief Finance Officer to discuss any concerns that come to light throughout the year.
- A member of the Executive Team (the Chief Finance Officer) is proactively and demonstrably responsible for tackling fraud, bribery and corruption.
There have been no assessments from the NHS Counter Fraud Authority, but should one occur an action plan would be taken forward following any recommendation made.
2.5. Head of Internal Audit Opinion
Following completion of the planned audit work for the period 1 April 2025 to 31 March 2026 for the ICB, the Head of Internal Audit issued an independent and objective opinion on the adequacy and effectiveness of the ICB’s system of risk management, governance and internal control. The Head of Internal Audit concluded that:
2.5.1. Head of Internal Audit Opinion
The organisation has an adequate and effective framework for risk management, governance and internal control. However, our work has identified further enhancements to the framework of risk management, governance and internal control to ensure that it remains adequate and effective.
2.5.2. Scope and limitations of our work
The formation of our opinion is achieved through a risk-based plan of work, agreed with management and approved by the audit committee, our opinion is subject to inherent limitations, as detailed below:
- Internal audit has not reviewed all risks and assurances relating to the organisation;
- The opinion is substantially derived from the conduct of risk-based plans generated from the ICB assurance framework. As such, the assurance framework is one component that the board takes into account in making its annual governance statement (AGS);
- The opinion is based on the findings and conclusions of the agreed work which was limited to the area under review and agreed with management and the lead individual.
- Where strong levels of control have been identified, there are still instances where these may not always be effective. This may be due to human error, incorrect management judgement, management override, controls being by-passed or a reduction in compliance.
- Due to the limited scope of our audits, there may be weaknesses in the control system which we are not aware of, or which were not brought to our attention.
- It remains management’s responsibility to develop and maintain a sound system of risk management, internal control and governance, and for the prevention and detection of material errors, loss or fraud. The work of internal audit should not be seen as a substitute for management’s responsibilities around the design and effective operation of these systems.
- The matters highlighted in this report represent only the issues we encountered during our work. It is not an exhaustive list of all weaknesses or potential improvements. Management remains responsible for maintaining a robust system of internal controls, and our work should not be the sole basis for identifying all strengths and weaknesses.
- This report is prepared solely for the use of the Board and Senior Management.
2.5.3. Factors and findings which have informed our opinion
Based on the work undertaken during 2025/26, there is generally a sound system of internal control, designed to meet the ICB’s objectives, and controls are generally being applied consistently, although there are some specific areas where improvements can be made.
We undertook the following Internal Audit reviews and issued the following reports:
| Assignment | Opinion |
| Data Security Protection Toolkit 24/25 (Cyber Assessment Framework ) | Low risk/ High Confidence |
| Recruitment IR35 & Consultants | Reasonable Assurance |
| Contract Management – GP Core Contracts (GMS & PMS) | Substantial Assurance |
| Quality & Equality Impact Assessments | Substantial Assurance |
| Financial Management | Reasonable Assurance |
| Transfer of Balances | Substantial Assurance |
| Data Security Protection Toolkit 25/26 (Cyber Assessment Framework ) | Low risk/ High Confidence |
| Finance Systems – Accounts Payable | Reasonable Assurance |
| Risk Management | DRAFT – Reasonable Assurance |
2.5.4. Topics judged relevant for consideration as part of the annual governance statement
Based on the work we have undertaken on the ICB’s system on internal control, there are no specific issues that we consider need to be flagged as significant control issues within the Annual Governance Statement (AGS).
2.5.5. Review of the effectiveness of governance, risk management and internal control within the Annual Governance Statement (AGS)
My review of the effectiveness of the system of internal control is informed by the work of the internal auditors, executive managers and clinical leads within the Integrated Care Board who have responsibility for the development and maintenance of the internal control framework. I have drawn on performance information available to me. My review is also informed by comments made by the external auditors in their annual audit letter and other reports.
Our assurance framework provides me with evidence that the effectiveness of controls that manage risks to the Integrated Care Board achieving its principles objectives have been reviewed.
I have been advised on the implications of the result of this review by:
- The Board
- The Audit and Risk committee
- Finance and Planning committee
- Quality and Oversight committee
- Internal audit
The role and conclusions of each were captured within the reports of the assurance committees to the Board.
2.5.6. Conclusion
No significant control issues have been identified at NHS South West London Integrated Care Board during 2025/26.

Andrew Bland
Chief Executive and ICB Accountable Officer
16 June 2026
2.6. Remuneration Report
2.6.1. Remuneration Committee
A summary of the duties and the membership of the remuneration committee is included within the governance section of the Annual Report.
2.6.2. Policy on the remuneration of senior managers
Remuneration for members, including the Accountable Officer and Chief Finance Officer, is determined based on reports to the Remuneration Committee, taking into account national guidance on pay rates, any independent evaluation of each post and national and market rates.
2.6.3. Remuneration of Very Senior Managers-Audited
The ICB has eight directors on a VSM grade who are paid more than £150,000 per annum. Their remuneration considers national guidance on pay rates, an independent evaluation of their post and national and market rates.
2.6.4. Senior manager remuneration (including salary and pension entitlements) 2025/26
The table below discloses salaries and allowances paid by the ICB to Directors of significant influence.
Percentage change in remuneration of highest paid director for 2025/2026:
| Salary and allowances | Performance pay and bonuses | |
| The percentage change from the previous financial year in respect of the highest paid director | -1.0% | N/A |
| The average percentage change from the previous financial year in respect of employees of South West London ICB, taken as a whole | -13.2% | N/A |
Percentage change in remuneration of highest paid director for 2024/2025:
| Salary and allowances | Performance pay and bonuses | |
| The percentage change from the previous financial year in respect of the highest paid director | 5.0% | N/A |
| The average percentage change from the previous financial year in respect of employees of South West London ICB, taken as a whole | -16.5% | N/A |
The calculation above in respect of employees of South West London ICB includes both permanent and interim staff, with their salary calculated on an annualised basis as a full-time equivalent employee.
2.6.5. Fair pay disclosure-Audited
Reporting bodies are required to disclose the relationship between the total remuneration of the highest-paid director / member in their organisation against the 25th percentile, median and 75th percentile of remuneration of the organisation’s workforce. Total remuneration of the employee at the 25th percentile, median and 75th percentile is further broken down to disclose the salary component.
The midpoint of the banded remuneration of the highest paid director (annualised) in SWL ICB in the reporting period 1st April 2025 to 31st March 2026 is shown below:
| Type | 2025/26 | 2024/25 |
| Midpoint of band of highest paid director | £247,500 | £247,500 |
The following table shows the 25th percentile, median and 75th percentile of total remuneration (excluding pension benefits), expressed as amounts, for the reporting entity’s staff (based on annualised full-time equivalent remuneration of all staff (including temporary and agency staff) for 2025/26:
| Remuneration measure for 2025/26 | 25th percentile | Median pay ratio | 75th percentile pay ratio |
| Total remuneration (£) | £46,764 | £60,651 | £80,837 |
| Salary component of total remuneration (£) | £46,764 | £60,651 | £80,837 |
The following table shows the 25th percentile, median and 75th percentile of total remuneration (excluding pension benefits), expressed as amounts, for the reporting entity’s staff (based on annualised full-time equivalent remuneration of all staff (including temporary and agency staff) for 2024/25:
| Remuneration measure for 2024/25 | 25th percentile | Median pay ratio | 75th percentile pay ratio |
| Total remuneration (£) | £45,352 | £62,189 | £82,576 |
| Salary component of total remuneration (£) | £45,352 | £62,189 | £82,576 |
The relationship to the remuneration of the organisation’s workforce is disclosed in the table below, which shows the ratios of staff remuneration against the remuneration of the highest paid director.
| Year | 25th percentile | Median pay ratio | 75th percentile pay ratio |
| 2025/26 | 5.29 | 4.08 | 3.06 |
| 2024/25 | 5.46 | 3.98 | 3.00 |
The following table shows the average salary per full time equivalent employee:
| Type | 2025/26 £000s | 2024/25 £000s |
| Total salary and allowances for all employees on an annualised basis, excluding the highest paid director | 55,341 | 63,743 |
| FTE number of employees (also excluding the highest paid director) | 662 | 645 |
| Average salary per FTE | 84 | 99 |
During the reporting period 2025/26, no employees received remuneration in excess of the highest-paid director/member (Annualised remuneration ranged from £3k to £247k).
Total remuneration includes salary, non-consolidated performance-related pay, benefits-in-kind, but not severance payments. It does not include employer pension contributions and the cash equivalent transfer value of pensions.
2.6.6. Senior manager remuneration (including salary and pension entitlements) – Audited
Senior manager remuneration between 1 April 2025 to 31 March 2026:
| Senior Manager | (a) Salary (bands of £5,000) £000′ | (b) Expense payments (taxable) to nearest £100** | (c) Performance pay and bonuses (bands of £5,000) £000′ |
| Mike Bell – Chair, Non-Executive Member, SWLICB | 25 to 30 | N/A | N/A |
| Anne Rainsberry – Non-Executive Member and Acting Chair, SWLICB | 40 to 45 | N/A | N/A |
| Sir Richard Douglas – Joint Chair, Non-Executive Member, SWL & SEL ICB’s | 5 to 10 | N/A | N/A |
| Jamal Butt – Non-Executive Member, SWLICB | 15 to 20 | N/A | N/A |
| Dr Masood Ahmed – Non-Executive Member, SWLICB | 15 to 20 | N/A | N/A |
| Martin Spencer – Non-Executive Member, SWLICB | 0 to 5 | N/A | N/A |
| Robert Alexander – Non-Executive Member, SWLICB | 15 to 20 | N/A | N/A |
| Omar Daniel – Associate Non-Executive Member, SWLICB | 5 to 10 | N/A | N/A |
| Katie Fisher – Chief Executive Officer, SWLICB | 205 to 210 | N/A | N/A |
| Andrew Bland – Chief Executive Officer, SWL & SEL ICB’s | 20 to 25 | N/A | N/A |
| Karen Broughton – Deputy CEO / Director of People & Transformation, SWLICB | 25 to 30 | N/A | N/A |
| Helen Jameson – Chief Finance Officer, SWLICB | 145 to 150 | N/A | N/A |
| Dinah McLannahan – Chief Finance Officer, SWLICB | 65 to 70 | N/A | N/A |
| Elaine Clancy – Chief Nursing Officer, SWLICB | 75 to 80 | N/A | N/A |
| Fergus Keegan – Acting Chief Nursing Officer, SWLICB | 80 to 85 | N/A | N/A |
| Dr John Byrne – Chief Medical Officer, SWLICB | 15 to 20 | N/A | N/A |
| Jonathan Bates – Chief Operating Officer, SWLICB | 95 to 100 | N/A | N/A |
| Jo Farrar – Partner Member, Community Services | 80 to 85 | N/A | N/A |
| Vanessa Ford – Partner Member, Mental Health Services (Note 2) | N/A | N/A | N/A |
| Cllr Andreas Kirsch – Partner Member, Local Authorities (Note 2) | N/A | N/A | N/A |
| Dr Nicola Jones – Partner Member, Primary Medical Services (Wandsworth GP) | 155 to 160 | N/A | N/A |
| Dame Cally Palmer – Partner Member, Specialised Services (Chief Executive Officer, The Royal Marsden NHS Foundation Trust) (Note 2) | N/A | N/A | N/A |
| Jacqueline Totterdell – Partner Member, Acute Services (Group Chief Executive Officer St George’s, Epsom and St Helier University Hospitals and Health Group) (Note 2) | N/A | N/A | N/A |
| James Blythe – Place Member, Sutton (Managing Director Epsom & St Helier NHS Trust) (Note 2) | N/A | N/A | N/A |
| Mark Creelman – Place Member, Wandsworth, SWLICB | 25 to 30 | N/A | N/A |
| Jeremy De Souza – Place Member, Richmond (Note 2) | N/A | N/A | N/A |
| Matthew Kershaw – Place Member, Croydon (Chief Executive Officer and Place Based Leader for Health Croydon Healthcare Services NHS Trust) | 20 to 25 | N/A | 0 to 5 |
| Dr Annette Pautz – Place Member, Kingston (Kingston GP) | 10 to 15 | N/A | N/A |
| Shannon Katiyo – Place Member, Merton (Note 2) | N/A | N/A | N/A |
| Senior Manager | (d) Long term performance pay and bonuses (bands of £5,000) £000′ | (e) All pension-related benefits (bands of £2,500) £000′ | (f) TOTAL (bands of £5,000) £000′ |
| Mike Bell – Chair, Non-Executive Member, SWLICB | N/A | N/A | 25 to 30 |
| Anne Rainsberry – Non-Executive Member and Acting Chair, SWLICB | N/A | N/A | 40 to 45 |
| Sir Richard Douglas – Joint Chair, Non-Executive Member, SWL & SEL ICB’s | N/A | N/A | 5 to 10 |
| Jamal Butt – Non-Executive Member, SWLICB | N/A | N/A | 15 to 20 |
| Dr Masood Ahmed – Non-Executive Member, SWLICB | N/A | N/A | 15 to 20 |
| Martin Spencer – Non-Executive Member, SWLICB | N/A | N/A | 0 to 5 |
| Robert Alexander – Non-Executive Member, SWLICB | N/A | N/A | 15 to 20 |
| Omar Daniel – Associate Non-Executive Member, SWLICB | N/A | N/A | 5 to 10 |
| Katie Fisher – Chief Executive Officer, SWLICB | N/A | N/A | 205 to 210 |
| Andrew Bland – Chief Executive Officer, SWL & SEL ICB’s | N/A | N/A | 20 to 25 |
| Karen Broughton – Deputy CEO / Director of People & Transformation, SWLICB | N/A | 10 to 12.5 | 35 to 40 |
| Helen Jameson – Chief Finance Officer, SWLICB | N/A | 0 | 145 to 150 |
| Dinah McLannahan – Chief Finance Officer, SWLICB | N/A | N/A | 65 to 70 |
| Elaine Clancy – Chief Nursing Officer, SWLICB | N/A | 75 to 77.5 | 150 to 155 |
| Fergus Keegan – Acting Chief Nursing Officer, SWLICB | N/A | 70 to 72.5 | 150 to 155 |
| Dr John Byrne – Chief Medical Officer, SWLICB | N/A | N/A | 15 to 20 |
| Jonathan Bates – Chief Operating Officer, SWLICB | N/A | 35 to 37.5 | 135 to 140 |
| Jo Farrar – Partner Member, Community Services | N/A | N/A | 80 to 85 |
| Vanessa Ford – Partner Member, Mental Health Services (Note 2) | N/A | N/A | N/A |
| Cllr Andreas Kirsch – Partner Member, Local Authorities (Note 2) | N/A | N/A | N/A |
| Dr Nicola Jones – Partner Member, Primary Medical Services (Wandsworth GP) | N/A | N/A | 155 to 160 |
| Dame Cally Palmer – Partner Member, Specialised Services (Chief Executive Officer, The Royal Marsden NHS Foundation Trust) (Note 2) | N/A | N/A | N/A |
| Jacqueline Totterdell – Partner Member, Acute Services (Group Chief Executive Officer St George’s, Epsom and St Helier University Hospitals and Health Group) (Note 2) | N/A | N/A | N/A |
| James Blythe – Place Member, Sutton (Managing Director Epsom & St Helier NHS Trust) (Note 2) | N/A | N/A | N/A |
| Mark Creelman – Place Member, Wandsworth, SWLICB | N/A | 7.5 to 10 | 35 to 40 |
| Jeremy De Souza – Place Member, Richmond (Note 2) | N/A | N/A | N/A |
| Matthew Kershaw – Place Member, Croydon (Chief Executive Officer and Place Based Leader for Health Croydon Healthcare Services NHS Trust) | N/A | N/A | 20 to 25 |
| Dr Annette Pautz – Place Member, Kingston (Kingston GP) | N/A | N/A | 10 to 15 |
| Shannon Katiyo – Place Member, Merton (Note 2) | N/A | N/A | N/A |
Senior manager remuneration between 1 April 2024 to 31 March 2025:
| Senior Manager | (a) Salary (bands of £5,000) £000′ | (b) Expense payments (taxable) to nearest £100** | (c) Performance pay and bonuses (bands of £5,000) £000′ |
| Mike Bell – Chair, Non-Executive Member, SWL Integrated Care Board | 50 to 65 | N/A | N/A |
| Anne Rainsberry – Non-Executive Member, SWL Integrated Care Board | 0 to 5 | N/A | N/A |
| Jamal Butt – Non-Executive Member, SWL Integrated Care Board | 5 to 10 | N/A | N/A |
| Masood Ahmed – Non-Executive Member, SWL Integrated Care Board | 5 to 10 | N/A | N/A |
| Martin Spencer – Non-Executive Member, SWL Integrated Care Board | 15 to 20 | N/A | N/A |
| Mercy Jeyasingham – Non-Executive Member, SWL Integrated Care Board | 10 to 15 | N/A | N/A |
| Dick Sorabji – Non-Executive Member, SWL Integrated Care Board | 0 to 5 | N/A | N/A |
| Ruth Bailey – Non-Executive Member, SWL Integrated Care Board | 5 to 10 | N/A | N/A |
| Robert Alexander – Associate Non-Executive Member | 0 to 5 | N/A | N/A |
| Omar Daniel – Associate Non-Executive Member | 0 to 5 | N/A | N/A |
| Katie Fisher – Chief Executive Officer, SWL Integrated Care Board From 17/02/25 | 25 to 30 | N/A | N/A |
| Sarah Blow – Chief Executive Officer, SWL Integrated Care Board To 16/02/25 | 245 to 250 | N/A | N/A |
| Karen Broughton – Deputy CEO / Director of People & Transformation, SWL Integrated Care Board | 165 to 170 | N/A | N/A |
| James Blythe – Place Member, Sutton (Managing Director Epsom & St Helier NHS Trust) (Note 3) | N/A | N/A | N/A |
| Cllr Ruth Dombey – Partner Member, Local Authorities (London Borough of Sutton) (To May 2024) (Note 3) | N/A | N/A | N/A |
| Elaine Clancy – Chief Nursing Officer, SWL Integrated Care Board | 160 to 165 | N/A | N/A |
| Dr John Byrne – Chief Medical Officer, SWL Integrated Care Board | 215 to 220 | N/A | N/A |
| Mark Creelman – Place Member, Wandsworth, SWL Integrated Care Board | 160 to 165 | N/A | N/A |
| Jeremy De Souza – Place Member, Richmond (Note 3) | N/A | N/A | N/A |
| Cllr Andreas Kirsch – Partner Member, Local Authorities (Note 3) | N/A | N/A | N/A |
| Vanessa Ford – Partner Member, Mental Health Services (Note 3) | N/A | N/A | N/A |
| Jo Farrar – Partner Member, Community Services (Note 1) | 75 to 80 | N/A | N/A |
| Helen Jameson – Chief Finance Officer, SWL Integrated Care Board | 185 to 190 | N/A | N/A |
| Dr Nicola Jones – Partner Member, Primary Medical Services (Wandsworth GP) | 135 to 140 | N/A | N/A |
| Matthew Kershaw – Place Member, Croydon (Chief Executive Officer and Place Based Leader for Health Croydon Healthcare Services NHS Trust) (Note 1) | 125 to 130 | N/A | 10 to 15 |
| Dame Cally Palmer – Partner Member, Specialised Services (Chief Executive Officer, The Royal Marsden NHS Foundation Trust) (Note 3) | N/A | N/A | N/A |
| Dr Annette Pautz – Place Member, Kingston (Kingston GP) | 65 to 70 | N/A | N/A |
| Jacqueline Totterdell – Partner Member, Acute Services (Group Chief Executive Officer St George’s, Epsom and St Helier University Hospitals and Health Group) (Note 3) | N/A | N/A | N/A |
| Shannon Katiyo – Place Member, Merton (Note 3) | N/A | N/A | N/A |
| Jonathan Bates – Participant, Chief Operating Officer, SWL Integrated Care Board | 160 to 165 | N/A | N/A |
| Charlotte Gawne – Executive Director of Stakeholder and Partnership Engagement and Communications, SWL ICB | 160 to 165 | N/A | N/A |
| Senior Manager | (d) Long term performance pay and bonuses (bands of £5,000) £000′ | (e) All pension-related benefits (bands of £2,500) £000′ | (f) TOTAL (bands of £5,000) £000′ |
| Mike Bell – Chair, Non-Executive Member, SWL Integrated Care Board | N/A | N/A | 60 to 65 |
| Anne Rainsberry – Non-Executive Member, SWL Integrated Care Board | N/A | N/A | 0 to 5 |
| Jamal Butt – Non-Executive Member, SWL Integrated Care Board | N/A | N/A | 5 to 10 |
| Masood Ahmed – Non-Executive Member, SWL Integrated Care Board | N/A | N/A | 5 to 10 |
| Martin Spencer – Non-Executive Member, SWL Integrated Care Board | N/A | N/A | 15 to 20 |
| Mercy Jeyasingham – Non-Executive Member, SWL Integrated Care Board | N/A | N/A | 10 to 15 |
| Dick Sorabji – Non-Executive Member, SWL Integrated Care Board | N/A | N/A | 0 to 5 |
| Ruth Bailey – Non-Executive Member, SWL Integrated Care Board | N/A | N/A | 5 to 10 |
| Robert Alexander – Associate Non-Executive Member | N/A | N/A | 0 to 5 |
| Omar Daniel – Associate Non-Executive Member | N/A | N/A | 0 to 5 |
| Katie Fisher – Chief Executive Officer, SWL Integrated Care Board From 17/02/25 | N/A | N/A | 25 to 30 |
| Sarah Blow – Chief Executive Officer, SWL Integrated Care Board To 16/02/25 | N/A | N/A | 245 to 250 |
| Karen Broughton – Deputy CEO / Director of People & Transformation, SWL Integrated Care Board | N/A | 22.5 to 25 | 190 to 195 |
| James Blythe – Place Member, Sutton (Managing Director Epsom & St Helier NHS Trust) (Note 3) | N/A | N/A | N/A |
| Cllr Ruth Dombey – Partner Member, Local Authorities (London Borough of Sutton) (To May 2024) (Note 3) | N/A | N/A | N/A |
| Elaine Clancy – Chief Nursing Officer, SWL Integrated Care Board | N/A | 42.5 to 45 | 205 to 210 |
| Dr John Byrne – Chief Medical Officer, SWL Integrated Care Board | N/A | N/A | 215 to 220 |
| Mark Creelman – Place Member, Wandsworth, SWL Integrated Care Board | N/A | 47.5 to 50 | 210 to 215 |
| Jeremy De Souza – Place Member, Richmond (Note 3) | N/A | N/A | N/A |
| Cllr Andreas Kirsch – Partner Member, Local Authorities (Note 3) | N/A | N/A | N/A |
| Vanessa Ford – Partner Member, Mental Health Services (Note 3) | N/A | N/A | N/A |
| Jo Farrar – Partner Member, Community Services (Note 1) | N/A | N/A | 75 to 80 |
| Helen Jameson – Chief Finance Officer, SWL Integrated Care Board | N/A | 192.5 to 195 | 380 to 385 |
| Dr Nicola Jones – Partner Member, Primary Medical Services (Wandsworth GP) | N/A | N/A | 135 to 140 |
| Matthew Kershaw – Place Member, Croydon (Chief Executive Officer and Place Based Leader for Health Croydon Healthcare Services NHS Trust) (Note 1) | N/A | N/A | 140 to 145 |
| Dame Cally Palmer – Partner Member, Specialised Services (Chief Executive Officer, The Royal Marsden NHS Foundation Trust) (Note 3) | N/A | N/A | N/A |
| Dr Annette Pautz – Place Member, Kingston (Kingston GP) | N/A | N/A | 65 to 70 |
| Jacqueline Totterdell – Partner Member, Acute Services (Group Chief Executive Officer St George’s, Epsom and St Helier University Hospitals and Health Group) (Note 3) | N/A | N/A | N/A |
| Shannon Katiyo – Place Member, Merton (Note 3) | N/A | N/A | N/A |
| Jonathan Bates – Participant, Chief Operating Officer, SWL Integrated Care Board | N/A | 20 to 22.5 | 180 to 185 |
| Charlotte Gawne – Executive Director of Stakeholder and Partnership Engagement and Communications, SWL ICB | N/A | 22.5 to 25 | 185 to 190 |
2.6.7. Pension benefits-Audited
Where the ICB contributed to pension schemes for senior managers, the benefits are shown in the tables below:
| Senior Manager | (a) Real increase in pension at pension age (bands of £2,500) £000 | (b) Real increase in pension lump sum at pension age (bands of £2,500) £000 | (c) Total accrued pension at pension age at 31 March 2025 (bands of £5,000) £000 | (d) Lump sum at pension age related to accrued pension at 31 March 2025 (bands of £5,000) £000 |
| Katie Fisher – Chief Executive Officer, SWL ICB | N/A | N/A | N/A | N/A |
| Andrew Bland – Chief Executive Officer, SWL & SEL ICB’s | N/A | N/A | N/A | N/A |
| Karen Broughton – Deputy CEO / Director of People & Transformation, SWLICB | 2.5 to 5 | 2.5 to 5 | 65 to 70 | 165 to 170 |
| Helen Jameson – Chief Finance Officer, SWLICB | 0 | 0 | 60 to 65 | 150 to 155 |
| Dinah McLannahan – Chief Finance Officer, SWLICB | N/A | N/A | N/A | N/A |
| Elaine Clancy – Chief Nursing Officer, SWLICB | 7.5 to 10 | 17.5 to 20 | 70 to 75 | 180 to 185 |
| Fergus Keegan – Acting Chief Nursing Officer, SWLICB | 5 to 7.5 | 10 to 12.5 | 50 to 55 | 125 to 130 |
| Dr John Byrne – Chief Medical Officer, SWLICB | N/A | N/A | N/A | N/A |
| Jonathan Bates – Chief Operating Officer, SWLICB | 2.5 to 5 | 2.5 to 5 | 70 to 75 | 170 to 175 |
| Mark Creelman – Place Member, Wandsworth, SWLICB | 2.5 to 5 | 0 | 40 to 45 | 0 |
| Senior Manager | (e) Cash Equivalent Transfer Value at 31 March 2024 £000 | (f) Real Increase in Cash Equivalent Transfer Value £000 | (g) Cash Equivalent Transfer Value at 31 March 2025 £000 | (h) Employers Contribution to partnership pension £000 |
| Katie Fisher – Chief Executive Officer, SWL ICB | N/A | N/A | N/A | N/A |
| Andrew Bland – Chief Executive Officer, SWL & SEL ICB’s | N/A | N/A | N/A | N/A |
| Karen Broughton – Deputy CEO / Director of People & Transformation, SWLICB | 1,480 | 74 | 1,600 | 24 |
| Helen Jameson – Chief Finance Officer, SWLICB | 1,352 | 0 | 1,348 | 21 |
| Dinah McLannahan – Chief Finance Officer, SWLICB | N/A | N/A | N/A | N/A |
| Elaine Clancy – Chief Nursing Officer, SWLICB | 1,438 | 201 | 1,686 | 26 |
| Fergus Keegan – Acting Chief Nursing Officer, SWLICB | 1,085 | 136 | 1,258 | 21 |
| Dr John Byrne – Chief Medical Officer, SWLICB | N/A | N/A | N/A | N/A |
| Jonathan Bates – Chief Operating Officer, SWLICB | 1,471 | 72 | 1,590 | 24 |
| Mark Creelman – Place Member, Wandsworth, SWLICB | 587 | 48 | 666 | 24 |
2.6.8. Cash equivalent transfer values- Audited
A cash equivalent transfer value (CETV) is the actuarially assessed capital value of the pension scheme benefits accrued by a member at a particular point in time. The benefits valued are the member’s accrued benefits and any contingent spouse’s (or other allowable beneficiary’s) pension payable from the scheme.
A CETV is a payment made by a pension scheme or arrangement to secure pension benefits in another pension scheme or arrangement when the member leaves a scheme and chooses to transfer the benefits accrued in their former scheme. The pension figures shown relate to the benefits that the individual has accrued as a consequence of their total membership of the pension scheme, not just their service in a senior capacity to which disclosure applies.
The CETV figures and the other pension details include the value of any pension benefits in another scheme or arrangement which the individual has transferred to the NHS pension scheme. They also include any additional pension benefit accrued to the member as a result of their purchasing additional years of pension service in the scheme at their own cost. CETVs are calculated within the guidelines and framework prescribed by the Institute and Faculty of Actuaries.
2.6.9. Real increase in CETV
This reflects the increase in CETV that is funded by the employer. It does not include the increase in accrued pension due to inflation or contributions paid by the employee (including the value of any benefits transferred from another scheme or arrangement).
2.6.10. Compensation on early retirement or for the loss of office
There were no payments for early retirement or loss of office.
2.6.11. Payments to past directors-Audited
There were no payments to past directors.
2.7. Staff Report
2.7.1. Number of senior managers
| Pay Band | Employee Headcount | FTE | Basic Annual Pay |
| Band 9 | 21 | 20.5 | £2,672,119 |
| VSM | 11 | 10.7 | £1,857,982 |
| Grand Total | 32 | 31.2 | £4,530,101 |
2.7.2. Staff numbers and costs-Audited
The following table shows the costs for permanently employed staff:
| Permanently employed staff | Cost, £000 | Average WTE |
| Add Prof Scientific and Technic | 4,126 | 41.6 |
| Administrative and Clerical | 45,615 | 494.2 |
| Allied Health Professionals | 204 | 2.1 |
| Medical and Dental | 3,527 | 17.0 |
| Nursing and Midwifery Registered | 5,818 | 67.2 |
| Total | 59,290 | 622.1 |
The following table shows the costs for other staff:
| Other staff (agency) | Cost, £000 | Average WTE |
| Add Prof Scientific and Technic | 0 | 0.0 |
| Administrative and Clerical | 2,444 | 17.3 |
| Allied Health Professionals | 0 | 0.0 |
| Medical and Dental | 1 | 0.0 |
| Nursing and Midwifery Registered | 1,914 | 23.6 |
| Total | 4,359 | 40.9 |
The following table shows the total costs for permanently employed staff and other staff:
| Total for Permanently employed staff and agency staff | Cost, £000 | Average WTE |
| Add Prof Scientific and Technic | 4,126 | 41.6 |
| Administrative and Clerical | 48,059 | 511.6 |
| Allied Health Professionals | 204 | 2.1 |
| Medical and Dental | 3,528 | 17.0 |
| Nursing and Midwifery Registered | 7,732 | 90.7 |
| Total | 63,649 | 663.0 |
The above table does not include any termination benefits included in the employee benefits and staff numbers note in the annual accounts.
2.7.3. Staff composition
2.7.3.1. Disability
| Disability flag | Headcount | % | FTE |
| No | 553 | 82.9 | 512.7 |
| Not Declared | 59 | 8.8 | 47.5 |
| Prefer Not to Answer | 10 | 1.5 | 9.3 |
| Yes | 45 | 6.7 | 42.5 |
| Grand Total | 667 | 100.0 | 612.0 |
2.7.3.2. Gender
| Gender | Headcount | % | FTE |
| Female | 475 | 71.2 | 438.2 |
| Male | 192 | 28.8 | 173.8 |
| Grand Total | 667 | 100.0 | 612.0 |
2.7.3.3. Sexual Orientation
| Sexual Orientation | Headcount | % | FTE |
| Bisexual | 6 | 0.9 | 6.0 |
| Gay or Lesbian | 17 | 2.5 | 16.9 |
| Heterosexual or Straight | 535 | 80.2 | 499.7 |
| Not stated or Person Declined | 104 | 15.6 | 84.5 |
| Other sexual orientation not listed | 2 | 0.3 | 2.0 |
| Undecided | 3 | 0.4 | 2.9 |
| Grand Total | 667 | 100.0 | 612.0 |
2.7.3.4. Employee Category (full or part time)
| Employee Category | Headcount | % | FTE |
| Full Time | 540 | 81.0 | 540.0 |
| Part Time | 127 | 19.0 | 72.0 |
| Grand Total | 667 | 100.0 | 612.0 |
2.7.3.5. Ethnicity Group
| Ethnicity Group | Headcount | % | FTE |
| White | 347 | 52.0 | 315.9 |
| BME | 278 | 41.7 | 262.4 |
| Not Stated | 42 | 6.3 | 33.8 |
| Grand Total | 667 | 100.00 | 612.0 |
2.7.3.6. Ethnicity
| Ethnic Group | Headcount | % | FTE |
| A White – British | 264 | 39.6 | 242.0 |
| B White – Irish | 21 | 3.1 | 20.8 |
| C White – Any other White background | 53 | 7.9 | 46.5 |
| C2 White Northern Irish | 1 | 0.1 | 0.1 |
| CA White English | 4 | 0.6 | 3.1 |
| CP White Polish | 1 | 0.1 | 1.0 |
| CY White Other European | 3 | 0.4 | 2.4 |
| D Mixed – White & Black Caribbean | 4 | 0.6 | 4.0 |
| E Mixed – White & Black African | 3 | 0.4 | 3.0 |
| F Mixed – White & Asian | 2 | 0.3 | 2.0 |
| G Mixed – Any other mixed background | 11 | 1.6 | 11.0 |
| H Asian or Asian British – Indian | 67 | 10.0 | 61.3 |
| J Asian or Asian British – Pakistani | 17 | 2.5 | 14.5 |
| K Asian or Asian British – Bangladeshi | 3 | 0.4 | 3.0 |
| L Asian or Asian British – Any other Asian background | 20 | 3.0 | 18.9 |
| LE Asian Sri Lankan | 1 | 0.1 | 0.4 |
| LF Asian Tamil | 2 | 0.3 | 1.4 |
| LH Asian British | 2 | 0.3 | 2.0 |
| LJ Asian Caribbean | 1 | 0.1 | 1.0 |
| LK Asian Unspecified | 2 | 0.3 | 1.3 |
| M Black or Black British – Caribbean | 33 | 4.9 | 31.9 |
| N Black or Black British – African | 73 | 10.9 | 71.9 |
| P Black or Black British – Any other Black background | 2 | 0.3 | 2.0 |
| PB Black Mixed | 1 | 0.1 | 1.0 |
| PD Black British | 3 | 0.4 | 2.6 |
| PE Black Unspecified | 1 | 0.1 | 0.9 |
| R Chinese | 12 | 1.8 | 10.9 |
| S Any Other Ethnic Group | 14 | 2.1 | 13.5 |
| SC Filipino | 3 | 0.4 | 3.0 |
| SD Malaysian | 1 | 0.1 | 1.0 |
| Z Not Stated | 42 | 6.3 | 33.8 |
| Grand Total | 667 | 100.00% | 612.0 |
2.7.3.7. Religion
| Religious Belief | Headcount | % | FTE |
| Atheism | 106 | 15.9 | 100.5 |
| Buddhism | 4 | 0.6 | 3.7 |
| Christianity | 258 | 38.7 | 244.6 |
| Hinduism | 46 | 6.9 | 40.9 |
| Islam | 36 | 5.4 | 33.1 |
| Jainism | 1 | 0.1 | 0.6 |
| Not Disclosed | 163 | 24.4 | 138.0 |
| Other | 39 | 5.8 | 37.4 |
| Sikhism | 14 | 2.1 | 13.2 |
| Grand Total | 667 | 100.00 | 612.0 |
2.7.3.6. Age Band
| Age Band | Headcount | % | FTE |
| <=20 Years | 1 | 0.1 | 0.4 |
| 21-25 | 4 | 0.6 | 3.4 |
| 26-30 | 31 | 4.6 | 30.2 |
| 31-35 | 62 | 9.3 | 59.8 |
| 36-40 | 91 | 13.6 | 86.0 |
| 41-45 | 99 | 14.8 | 90.3 |
| 46-50 | 114 | 17.1 | 100.4 |
| 51-55 | 96 | 14.4 | 88.4 |
| 56-60 | 96 | 14.4 | 90.4 |
| 61-65 | 53 | 7.9 | 47.0 |
| 66-70 | 14 | 2.1 | 11.0 |
| >=71 Years | 6 | 0.9 | 4.7 |
| Grand Total | 667 | 100.00 | 612.0 |
2.7.3.9. Marital Status
| Marital Status | Headcount | % | FTE |
| Civil Partnership | 10 | 1.5 | 10.0 |
| Divorced | 28 | 4.2 | 26.8 |
| Legally Separated | 4 | 0.6 | 3.9 |
| Married | 314 | 47.1 | 280.8 |
| Single | 210 | 31.5 | 203.5 |
| Unknown | 97 | 14.5 | 83.9 |
| Widowed | 4 | 0.6 | 3.1 |
| Grand Total | 667 | 100.00 | 612.0 |
2.7.4. Sickness absence data
Our sickness absence percentage rate is presented regularly to the ICB in the form of workforce reports. Individual sickness absence cases are managed by the line manager with advice and support from HR.
An occupational health service is available to provide professional clinical advice to line managers within the ICB.
We also have access to an employee assistance programme which offers confidential access to emotional and practical support, including legal and financial advice.
| Adjusted FTE days Lost | 4,579 |
| Average FTE for 2025 | 617 |
| Average Sick Days per FTE | 7 |
2.7.5. Staff turnover percentages
The annual average full-time staff turnover rate for 2025/26 was 14.29%. The equivalent figure for 2024/25 was 16.55%.
2.7.6. Staff communications and engagement
Staff communications and engagement remained a top priority as we supported our staff through the NHS Changes programme while continuing to deliver services to support local people.
Throughout the year, we continued to provide clear and effective communications, including:
- online all staff briefings led by our Chief Executive Officer, who shares and discusses the latest NHS and South West London priorities with a strong focus on the NHS Change programme.
- monthly Team Talk meetings led by executive directors who discuss organisational news and updates and celebrate our achievements.
- support to line managers to ensure they are equipped to support their staff during the management cost savings process.
- a weekly email bulletin which provides news and workforce updates.
- ServiceNow online portal – where staff can find all the latest news and updates, policies, learning and development opportunities, and health and wellbeing support.
2.7.7. NHS Staff Survey
NHS South West London commissioned Picker Institute Europe to run a National Staff Survey for us locally during September and October 2025. The ICB had a score of 6.29 for Staff Engagement which was lower than our 2024 score of 6.41. For comparison, the average ICB score across the country was 6.28.
A total of 327 took part in the survey, giving a response rate of 49%, considerably lower than the previous year’s response rate of 75%. This was expected given the circumstances of the NHS changes ICBs are undergoing. We are grateful to everyone who took the time to complete the survey.
The results of the survey were published in March 2026. The majority of results have not significantly changed compared to the previous year, however, there are several areas where we recognise improvements are needed for our staff.
2.7.7.1. Where we’re doing well
| Most improved scores | 2025 | 2024 |
| Q23a. Received appraisal in the past 12 months | 90% | 52% |
| Q7d. Team members understand each other’s roles | 63% | 52% |
| Q24f. Able to access clinical supervision opportunities | 48% | 37% |
| Q231b. Disability: organisation made reasonable adjustment(s) to enable me to carry out work | 76% | 66% |
| Q23g. Able to meet conflicting demands on my time at work | 53% | 44% |
2.7.7.2. Where we’re doing less well
| Most declined scores | 2025 | 2024 |
| Q26b I am unlikely to look for a job at a new organisation in the next 12 months | 26% | 37% |
| Q11d In last 3 months, have not come to work when not feeling well enough to perform duties | 45% | 55% |
| Q26c I am not planning on leaving this organisation | 36% | 45% |
| Q12g Never/rarely lack energy for family and friends | 37% | 45% |
| Q25c Would recommend organisation as place to work | 41% | 49% |
Given the current changes taking place within the ICB, we plan to use our analysis of these staff survey results alongside the findings from our interactive sessions with staff to make sure we are best supporting our staff over the coming months.
You can read more about the NHS staff survey on the NHS staff survey website.
2.7.8. Staff policies
We promote a working environment in which we aim to ensure all policies and procedures relating to recruitment, selection, training, promotion and employment are free from discrimination, ensuring that no employee or prospective employee is discriminated against, whether directly or indirectly on the grounds of age; disability; gender reassignment; pregnancy and maternity; race including ethnic or nationality; religious belief; sex (gender); sexual orientation; disability; marriage and civil partnership status; trade union membership; responsibility for dependents or any other characteristic identified legally as protected in the Equality Act 2010 or through any other relevant legislation.
We endeavour to make sure that the requirements and reasonable adjustments necessary for employees with a disability are considered both during each stage of the recruitment process and during employment.
The Freedom to Speak Up Policy sets out our commitment to fostering an open and honest culture where staff feel safe and supported to raise concerns. This policy was one of a number of recommendations of the review by Sir Robert Frances into whistleblowing in the NHS, aimed at improving the experience of whistleblowing in the NHS. The Audit Committee receives reports on Freedom to Speak Up at each of its meetings and our Freedom to Speak Up Guardian also updates the senior management team every month.
Our Sickness Absence Policy confirms that where an employee becomes disabled during their employment, we will support them with occupational health advice and to see if any reasonable adjustments will enable the employee to return and remain at work in accordance with the Equality Act. The types of adjustments may include adjustments to work base, working hours, redeploying the employee to another suitable position, and providing any necessary equipment to assist the employee to perform their role.
We have centralised our people policies ensuring they have gone through the Equality Impact process to ensure there are fair outcomes for our workforce, and that they meet the accessibility standards. We are also in the process of working closely with NHS South East London to align our policies where possible, in particular the Change Management Policy in light of our cluster arrangements.
2.7.9. Other employee matters
We have continued to provide regular health and wellbeing support and guidance to staff, which is particularly important during the NHS Changes programme. We include health and wellbeing support updates in our weekly update, all staff briefings, and Team Talk.
We continue to make progress against our equality delivery plan objectives. Details of this can be found in our public sector equality duty (PSED) report for this year.
2.7.10. Expenditure on consultancy
The reported expenditure on consultancy in 2025/26 was £83k (£252k in 2024/25).
2.7.11. Off-payroll engagements
2.7.11.1. Off-payroll engagements longer than six months
For all off-payroll engagements as of 31 March 2026 for more than £245* per day and that lasted longer than six months:
| Off-payroll engagements | Number |
| Number of existing engagements as of 31 March 2026 | 29 |
| Off-payroll engagements of which, the number that have existed: | Number |
| for less than one year at the time of reporting | 21 |
| for between one and two years at the time of reporting | 5 |
| for between 2 and 3 years at the time of reporting | 2 |
| for between 3 and 4 years at the time of reporting | 0 |
| for 4 or more years at the time of reporting | 1 |
*The £245 threshold is set to approximate the minimum point of the pay scale for a Senior Civil Servant.
All existing off-payroll engagements have at some point been subject to a risk-based assessment as to whether assurance is required that the individual is paying the right amount of tax and, where necessary, that assurance has been sought.
2.7.11.2. Off-payroll workers engaged at any point during the financial year
For all off-payroll engagements between 1 April 2025 and 31 March 2026, for more than £245(1) per day:
| Off-payroll engagements | Number |
| No. of temporary off-payroll workers engaged between 1 April 2025 and 31 March 2026 | 92 |
| Off-payroll engagements of which | Number |
| No. not subject to off-payroll legislation (2) | 1 |
| No. subject to off-payroll legislation and determined as in-scope of IR35 (2) | 88 |
| No. subject to off-payroll legislation and determined as out of scope of IR35 (2) | 3 |
| the number of engagements reassessed for compliance or assurance purposes during the year | 0 |
| Of which: no. of engagements that saw a change to IR35 status following review | 0 |
(1) The £245 threshold is set to approximate the minimum point of the pay scale for a Senior Civil Servant.
(2) A worker that provides their services through their own limited company or another type of intermediary to the client will be subject to off-payroll legislation and the Department must undertake an assessment to determine whether that worker is in-scope of Intermediaries legislation (IR35) or out-of-scope for tax purposes.
2.7.11.3. Off-payroll engagements / senior official engagements
For any off-payroll engagements of Board members and / or senior officials with significant financial responsibility, between 1 April 2025 and 31 March 2026:
| Off-payroll engagements | Number |
| Number of off-payroll engagements of board members, and/or senior officers with significant financial responsibility, during reporting period(1) | 0 |
| Total no. of individuals on payroll and off-payroll that have been deemed “board members, and/or, senior officials with significant financial responsibility”, during the reporting period. This figure should include both on payroll and off-payroll engagements. (2) | 12 |
(1) There should only be a very small number of off-payroll engagements of board members and/or senior officials with significant financial responsibility, permitted only in exceptional circumstances and for no more than six months.
(2) As both on payroll and off-payroll engagements are included in the total figure, no entries here should be blank or zero. In any cases where individuals are included within the first row of this table the ICB should set out.
2.7.11.4. Exit packages, including special (non-contractual) payments- Audited
These tables report the number and value of exit packages agreed in the financial year.
| Exit package cost band (including any special payment element) | Number of compulsory redundancies (Whole Numbers Only) | Cost of compulsory redundancies (£s) | Number of other departures agreed (Whole Numbers Only) | Cost of other departure agreed (£s) | Total number of exit packages (Whole Numbers Only) | Total costs of exit packages (£s) | Number of departures where special payments have been made (Whole Numbers Only) | Cost of special payment element included in exit packages (£s) |
| Less than £10,000 | 1 | 1,259 | 4 | 31,161 | 5 | 32,420 | 0 | 0 |
| £10,000 – £25,000 | 1 | 12,998 | 11 | 189,292 | 12 | 202,290 | 0 | 0 |
| £25,001 – £50,000 | 0 | 0 | 34 | 1,267,243 | 34 | 1,267,243 | 0 | 0 |
| £50,001 – £100,000 | 0 | 0 | 45 | 3,407,346 | 45 | 3,407,346 | 0 | 0 |
| £100,001 – £150,000 | 1 | 137,292 | 38 | 4,697,005 | 39 | 4,834,298 | 0 | 0 |
| £150,001 – £200,000 | 2 | 359,000 | 31 | 5,187,204 | 33 | 5,546,204 | 0 | 0 |
| >£200,000 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Totals | 5 | 510,550 | 163 | 14,779,250 | 168 | 15,289,800 | 0 | 0 |
2.8. Parliamentary Accountability and Audit Report
NHS South West London Integrated Care Board is not required to produce a Parliamentary Accountability and Audit Report.
Disclosures on remote contingent liabilities, losses and special payments, gifts, and fees and charges are included as notes in the Financial Statements of this report. An audit certificate and report are also included in this Annual Report.

Andrew Bland
Chief Executive and ICB Accountable Officer
16 June 2026